Carmen Jiménez-Gutiérrez ¹ , Marina Pérez-del-Rincón ² , Pablo Reduello-Guerrero ² , Marta Presentación Rodríguez-
Rodríguez ² , Ana María Toral-López ² , Clara Amanda Ureña-Paniego ²
1 Estudiante del Grado en Enfermería de la Universidad de Granada (UGR)
2 Estudiante del Grado en Medicina de la Universidad de Granada (UGR)
TRANSLATED BY:
Celia Morales-García ³ , María Auxiliadora Camacho-Martí ³ , Kathryn Sword ³ , Gudrun Palomino-Tirado ³ , Pablo Diego
Torregrosa-Parra ³ , Elena Company-Campos ³
3 Student of the BA in Translation and Interpreting at the University of Granada (UGR)
TRADUCCIÓN ÁRABE: Nuria Calvo-Cano ³ , Zakaría Abdessadak ³ , Doae Haourigui ³ , Sonia Hayaoui-Aomar ³ , Khitam El-Kenfaoui ³ , Paula Bulpe-Nieto ³
3طلبة الترجمة التحريرية والشفوية في جامعة غرناطة.
Resumen
Cada año, se producen más de 15 millones de partos prematuros, de los cuales, una fracción considerable es ingresada en la unidad de cuidados intensivos neonatales. La conjunción de un período crítico en el desarrollo neurocognitivo, el aislamiento parental y un entorno hostil hacen de estos pacientes una población vulnerable a diferentes discapacidades de tipo cognitivo, motor, lingüístico, comportamental y socio-económico, que también afecta a su entorno. Por ello, se proponen la musicoterapia y la terapia musical como alternativas no invasivas en aras de mejorar las variables relacionadas con nutrición, respuestas de dolor y estrés, parámetros fisiológicos del neonato, así como de lactancia materna.
Palabras clave: música, sonido, parto pretérmino, unidad cuidados intensivos neonatales, no invasivo, revisión.
Keywords: music, sound, preterm birth, neonatal intensive care unit, non-invasive, review.
- INTRODUCCIÓN
Se
define al recién nacido prematuro como a todo aquel “que nace antes de
completar la semana 37 de gestación” (1). Cada año, se producen más de 15
millones de partos prematuros, constituyendo 1 de cada 10 nacimientos. La tasa
de partos prematuros presenta una tendencia ascendente a nivel mundial (2). A
pesar de que las mejoras tecnológicas están incrementando la supervivencia de
esta población. Un parto prematuro puede afectar al desarrollo cognitivo,
motor, lingüístico, comportamental y socio-económico del infante, así como al
estado de salud mental de la familia, especialmente de la madre (3). Una
proporción importante de estos infantes precisan de cuidados intensivos para
sobrevivir fuera del entorno intrauterino. Es por ello que la Unidad de
Cuidados Intensivos Neonatales (UCIN) se convierte en la fuente de los primeros
estímulos para estos prematuros. Estas unidades se caracterizan por el alto
número de procedimientos invasivos (y por consiguiente, dolorosos y
estresantes) así como por el aislamiento parental a los que se ven sometidos
los pacientes (4). Estos sucesos acontecen durante una época de desarrollo
cerebral temprano, que se caracteriza por la formación de conexiones
sinápticas, desarrollo de espinas dendríticas, mielinización axonal y
plegamiento neocortical (5,6). Diversos estudios apuntan a que el sistema del
infante prematuro posee ya capacidad anatómica y neuroquímica de la percepción
del dolor (4), por lo que los prematuros ingresados en la UCIN parecen un grupo
especialmente susceptible para la disrupción de estos hitos del
neurodesarrollo. A esto se le suma la activación de la respuesta de estrés por
medio del eje hipotálamo hipofisario adrenal y del sistema simpático, que
condicionan respuestas fisiológicas representativas de la reacción dual de
“lucha o huida”. Entre éstas, se encuentra el aumento de la frecuencia cardíaca
y respiratoria y el aumento del cortisol, respuestas cuya puesta en marcha desvían
recursos energéticos del sistema nervioso en formación (6). Asimismo, la leche
humana se considera en la actualidad como uno de los factores claves en la
mejora del paciente pretérmino durante su hospitalización en la UCIN, así como
el estándar de cuidado en esta misma unidad (7). Desafortunadamente, la
hospitalización en la UCIN supone para los padres un evento potencialmente
traumático. La importancia de este hecho deriva de la asociación indefectible
entre estrés físico y mental y reducción de la eyección de leche por
disminución de los niveles de oxitocina durante la lactancia (8).
Bajo
la premisa de numerosos estudios que demuestran que la música puede mejorar de
manera no invasiva el desenlace de estos infantes, se contempla la utilización
de la musicoterapia y la terapia musical como instrumentos no invasivos para la
mejora de estos resultados (6). En la presente revisión se distinguirá entre
los conceptos de terapia musical (TM) y estimulación musical (EM). Según la
Asociación Americana de Musicoterapia, la primera se define como “aquellas
intervenciones clínicas y basadas en la evidencia que hacen uso de la música
para alcanzar metas individuales en el contexto de una relación terapéutica
realizada por un profesional acreditado” (9). Por otro lado, la EM la
constituyen “aquellas intervenciones desarrolladas por un sanitario o los
padres del infante”. Esta revisión narrativa persigue examinar los beneficios
de la MT y la EM sobre las funciones vitales del prematuro como son la
nutrición y estado general de salud, reflejado en duración de la estancia
hospitalaria y parámetros fisiológicos, así como indicadores de dolor y
lactancia materna.
2. NUTRICIÓN DEL INFANTE PRETÉRMINO
En cuanto a la alimentación, se ha observado que la MT ayuda a los
niños prematuros en la UCIN a sustituir progresivamente la alimentación por vía
intravenosa a alimentación por vía oral. El uso de un reproductor de música con
canciones cantadas por la madre favorece de forma significativa el cambio de
alimentación. Se vio que en el 94 % de los niños a los que se les estimuló con
un reproductor con grabaciones de voz materna se consiguió una alimentación
completa por vía oral en al menos 7 días antes que en los niños a los que se
les ponía un tranquilizante estándar o que escuchaban la voz de la madre solo
en algunas ocasiones (10). No obstante, no se encontraron diferencias
significativas en cuanto al aumento de peso entre el grupo de intervención y el
grupo control. Cabe resaltar que otros
estudios apuntan a que la estimulación oral presenta mejores resultados en la
mejora de la alimentación del prematuro que la estimulación auditiva (con
canciones de cuna). No obstante, los prematuros que tenían estimulación
auditiva mejoraron más que los del grupo control a los que no se le aplicaba
ninguna intervención a excepción de los cuidados rutinarios (11). Las
diferencias en estos grupos fueron significativas, encontrándose que el grupo
con estimulación oral alcanzaba la alimentación por vía oral completa en un
periodo más corto de tiempo que los que recibieron la estimulación auditiva.
Finalmente, los niños del grupo control que no tuvieron intervención fueron los
que más tiempo tardaron en alcanzar este tipo de alimentación de forma
completa. En relación con estos datos, también se encontraron diferencias en la
capacidad de succión de los distintos grupos, la cual iba relacionada con la
mejora de la alimentación por vía oral.
En algunas revisiones se consideraron las posibles diferencias en los
resultados obtenidos en función de si se realizaba una exposición a música en
vivo o una exposición con un reproductor musical. Se apunta a que ambos tipos
de TM aumentan la capacidad de succión de los recién nacidos prematuros y
disminuyen el tiempo necesario para alcanzar una alimentación por vía oral
completa (3). Otros estudios apuntan a que la música en vivo ayuda al prematuro
a conciliar un sueño más profundo que el uso de un reproductor musical (12). El
tipo de música también influye en la mejora de los neonatos prematuros. Se ha
visto que las canciones de cuna ayudan a mejorar la alimentación por vía oral y
también a aumentar la ingesta calórica diaria del infante. Además, el uso de
reproductores musicales con canciones cantadas por la madre aumenta de forma
considerable la alimentación por vía oral frente a otros métodos de EM (13).
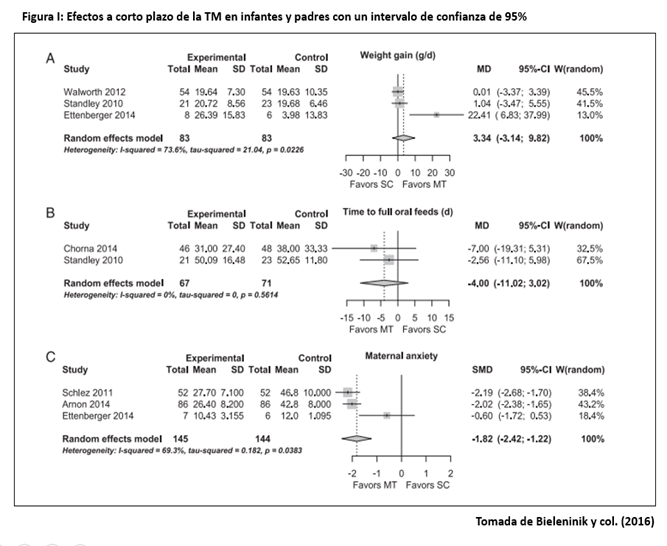
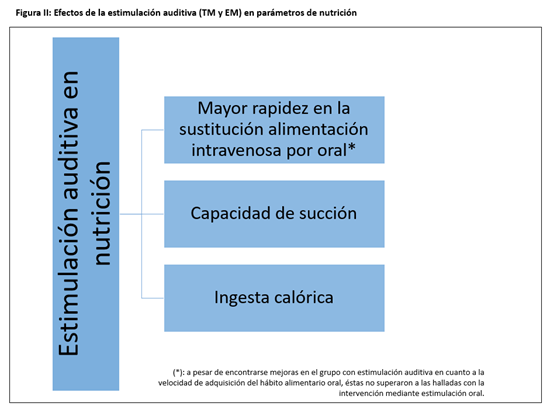
La figura I resume los hallazgos más representativos de la TM y EM sobre la nutrición neonatal en pretérminos.
3. COMPORTAMIENTOS DE DOLOR Y ESTRÉS
Los prematuros, principalmente aquellos que
ingresan en UCIN, suelen encontrarse durante su estancia hospitalaria en un
ambiente estresante y sobreestimulante. Además, son expuestos a numerosos
procedimientos dolorosos, tanto diagnósticos como terapéuticos. Todo esto
acarrea consecuencias adversas para su posterior desarrollo neurológico y del
sistema de percepción del dolor, así como alteraciones fisiológicas negativas
(6,14-15). Los efectos negativos de algunos analgésicos y su mal uso junto a la
en ocasiones excesiva duración de sus efectos hacen que los métodos no
farmacológicos como la MT sean una alternativa cada vez más usada (16). Aunque hay muchos estudios referentes a la
musicoterapia en neonatos y prematuros, suelen centrarse en el comportamiento y
la estimulación del desarrollo, y pocos de ellos investigan la respuesta al
dolor (14) y el estrés, a pesar de que algunos valoran parámetros relacionados
con ambos. En algunos ensayos aleatorizados controlados, todos referentes a la
“prueba del talón”, se observó un descenso del
dolor medido en las escalas Neonatal Infant
Pain Scale (NIPS) y Neonatal Facial
Coding Sistem (NFCS), y FR, aumento de la presión parcial de oxígeno
transcutánea (TcPaO2) y efectos significativos en el comportamiento. Los
neonatos con más de 31 semanas de vida podrían beneficiarse más de estos
efectos, sobre todo en los momentos posteriores al procedimiento (17). La
razón, según señalan algunos autores podría estar en su mayor desarrollo, que
permitiría una mayor respuesta al estímulo musical (14).
En cuanto al tipo y la forma de aplicación de
la música, solo se han estudiado grabaciones, siendo estas de música clásica,
pulsos maternos intrauterinos con música relajante, nanas, incluyendo PAL. La
música clásica no ha tenido resultados positivos significativos, ni ha
conseguido mejorar el efecto beneficioso del amamantamiento, así como la PAL no
ha tenido efecto en el dolor, solo en el estrés y el comportamiento. Las nanas
se recomiendan por tener menores variaciones en su melodía, y se aconseja también
el uso de música en vivo. No hay resultados comparables acerca del volumen de
la música, si bien se pueden seguir algunas recomendaciones sobre ruido en UCIN
no concretadas en la MT, como evitar superar los 45dB. Se ha sugerido también
que la aplicación conjunta con otros métodos no farmacológicos, como la sucrosa
o la succión no nutritiva, tendría mayores efectos positivos que la aplicación
aislada de musicoterapia, a excepción del amamantamiento como se ha mencionado
anteriormente.
Como conclusión, la musicoterapia podría tener
efectos beneficiosos en el manejo del dolor procedimental de prematuros en UCI
y puede ser usada para este fin, pero hay muy pocos estudios al respecto, con
poca muestra y con variables muy heterogéneas, como para establecer indicaciones
prácticas concretas al respecto. En relación al estrés, si bien se han
demostrado mejoras en los parámetros fisiológicos, sería necesario hacer más
estudios con mediciones objetivas de la activación del sistema
hipotálamo-pituitaria-adrenal (6).
4.
PARÁMETROS FISIOLÓGICOS
Tras
diversos estudios realizados en distintas partes del mundo (España entre ellas)
se ha demostrado el impacto de la TM en los nacidos prematuramente en sus
parámetros fisiológicos. En este
apartado se comentarán múltiples estudios realizados con distintos tamaños de
muestra. En el primer caso a estudiar se analizan 12 prematuros tratados con
TM, 8 de los cuales obtienen resultados beneficiosos en varios aspectos
fisiológicos. Evaluando individualmente,
se extraen las siguientes conclusiones:
- En 3 de ellos se constata que la
música mejora a corto plazo la frecuencia cardíaca (FC) y la saturación de
oxígeno (SpO2). - En 5 casos de neonatos se usó la
música clásica, siendo concretamente la música de Mozart la más efectiva.
También se evalúa la respuesta con la voz materna, obteniendo en 2 infantes una
mejora de los niveles de SpO2 (13).
En la
revisión sistemática elaborada por van der Heijden y colaboradores (18) se revisaron 20 estudios, en los que se
valoraron distintas categorías de resultados. De éstos, 14 evaluaban el efecto
de la TM y la EM sobre la FC, la frecuencia respiratoria (FR), la SpO2 y los
niveles de cortisol. De este análisis se extrae que en 7 de los 12 casos que
utilizaron música grabada, no hubo diferencias significativas. Sin embargo,
entre el resto podemos encontrar diferencias significativas en:
- Aumento de la SpO2.
- Disminución de la FC y FR durante
y después de la TM.
Por
último, en cuatro estudios, en los que se midió el efecto de la música en
directo, los revisores concluyeron que se producen diferencias significativas
en dos de ellos en cuanto a la reducción de la FC, pero no significativas en
los otros dos.
Otra
investigación consistió en un análisis de diferentes parámetros en neonatos en
dos hospitales españoles, antes y tras la intervención de 20 minutos de música
relajante, 3 veces al día durante 3 días consecutivos. Este estudio concluyó
que la utilización de música relajante mejora parámetros fisiológicos durante
la hospitalización, sin efectos negativos. El grupo de intervención obtiene
mejoras en FC y FR, mientras que no hubo cambios significativos en la SpO2 y
presión sanguínea (19). De igual forma, diversos estudios parecen señalar a
mejoras en los parámetros fisiológicos de los neonatos prematuros
hospitalizados causadas por TM. En uno de ellos se especifica que el
tratamiento con música en dichos neonatos reduce 3.91 respiraciones por minuto.
Con respecto a la FC no se consideró el resultado como significativo, aunque el
autor lo atribuye al alto sonido de las grabaciones utilizadas en la evaluación
de la intervención (20).
Como
conclusión de todos los estudios realizados en distintos casos, se observa la
notable mejora general de la FC y FR del nacido de manera precoz, así como
aumentos en la SpO2, tras intervenciones de TM y EM en prematuros
hospitalizados (3). Los hallazgos más relevantes del metaanálisis contemplado
quedan resumidos en la figura I.
5. LACTANCIA MATERNA
La
lactancia materna supone un gran beneficio para los recién nacidos ya que es un
alimento natural que cubre todas sus necesidades nutricionales en sus primeros
meses de vida. Está compuesta por las cantidades adecuadas de hidratos de
carbono, proteínas, grasas, minerales, vitaminas, enzimas digestivas, hormonas
y anticuerpos. Es por ello que este acontecimiento adquiere más importancia en
los infantes pretérmino, debido a que nacen más inmaduros por la reducción del
período gestacional, lo que incrementa el riesgo de padecer diversas
enfermedades. Además, los ingresados en la UCIN necesitan un aporte nutricional
de calidad superior al recién nacido a término. Por este motivo, es necesario
que sus madres se encuentren en las óptimas condiciones para amamantarlos. La
realidad, no obstante, muestra que el alto nivel de estrés al que se ven
sometidas las madres en la UCIN junto con las dificultades fisiológicas
derivadas de un desarrollo incompleto de los mecanismos de lactancia maternos,
reduce la calidad y cantidad de leche que la madre es capaz de expulsar.
Es
necesario que los servicios sanitarios lleven a cabo medidas de apoyo a la
lactancia enfocadas, por ejemplo, desde la MT. Este tipo de terapias durante
las sesiones de lactancia ayudan a reducir el estrés que sufren estas madres
influyendo en la mejora de la producción tanto del contenido en grasa como del
volumen de leche materna, aunque no hay evidencia de que afecte a los niveles
de oxitocina (21). Por otro lado, sí que se ha demostrado que la TM disminuye
los niveles de cortisol, marcador del estrés así como la FR, presión arterial y
de la temperatura de los dedos así como la relajación percibida en la lactante
(22-23). Las técnicas de relajación
acompañadas de imágenes de sus recién nacidos provocan en la madre una
mejora de la actividad secretora, constituyendo una técnica que no es invasiva
para madre ni para el infante, constituyendo la TM uno de los mecanismos más
accesibles (21). Asimismo, este tipo de terapias tienen el beneficio de poderse
realizar tras el alta médica y no supone un alto coste. También, la elección
por parte de las madres de la música escuchada ha podido evidenciar una mejora
en la producción de la leche al igual que su implicación en alguna actividad
con la música. A su vez, compaginar la musicoterapia con el yoga, la relajación
muscular progresiva, imágenes guiadas y otras ha dado mejores resultados en la
reducción del estrés de la madre y como consecuencia en la mejora de la
lactancia (21,23-24).
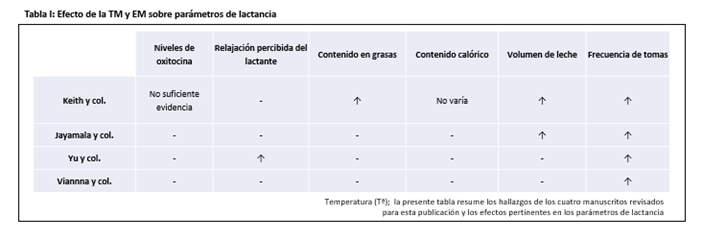
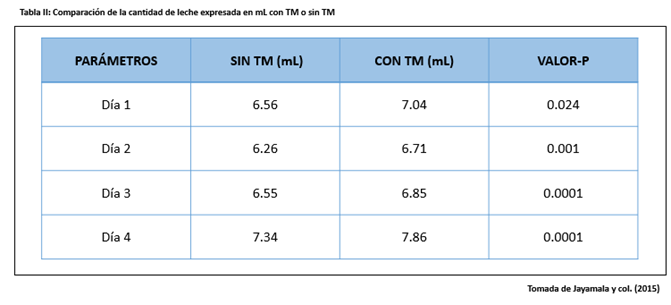
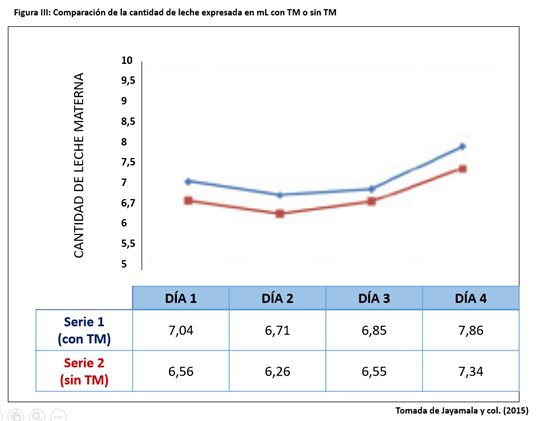
En conclusión, y tal y como recogen las figuras II y III, así como las tablas I y II, la lactancia supone para el infante (aún más siendo pretérmino) como para la madre amplios beneficios tanto psicológicos como físicos. Así que, es importante que, junto con la educación sanitaria para favorecer la lactancia, se proporcionen a las madres actividades e intervenciones como la TM con el propósito de reducir su estrés, ayudar a mejorar la producción y calidad de la leche y favorecer la diada madre-hijo en situaciones tan delicadas como el ingreso del recién nacido en la UCIN.
6. CONCLUSIÓN
El
objeto de esta revisión era examinar los resultados publicados hasta la fecha
sobre TM y EM y su impacto en la salud de infantes prematuros y lactancia en el
entorno de la UCIN. La mayor parte de los estudios y revisiones parecen indicar
que la TM y la EM afectan de manera positiva a parámetros de alimentación, de
dolor y estrés, fisiológicos y de lactancia.
No obstante, debido a la gran heterogeneidad de intervenciones,
metodología, análisis de datos y evaluaciones de resultados encontradas, así
como la ausencia de un seguimiento consistente y a largo plazo, se recomienda
cautela a la hora de aceptar la validez de los resultados arrojados. Asimismo,
se ha observado como factor común que la MT y EM pueden actuar sinérgicamente a
otros procedimientos y técnicas de relajación, por lo que futuras
investigaciones podrían explorar la eficacia de intervenciones combinadas
comparadas con las intervenciones individuales.
Independientemente
de la significación clínica o no de los efectos de estas terapias, su inocuidad
y bajo coste hacen de la TM y la EM una herramienta innovadora y con indicios
prometedores a la hora de mejorar la calidad de los prematuros ingresados en la
UCIN, así como la de sus familias. La hospitalización y estancia de infantes
pretérmino en estas unidades constituye una situación crítica que exige los
mejores cuidados posibles y la ciencia más rigurosa.
Conflicto de intereses: los
autores declaran no tener ningún conflicto de interés.
7. REFERENCIAS
1. Rellan Rodríguez S, García de Ribera C, Aragón García MP. El recién nacido prematuro. Madrid: Asociación Española de Pediatría; 2008 [Last accesed 15 March 2019]. Available at: http://www.aeped.es/sites/default/files/documentos/8_1.pdf
2. P Howson, MV Kinney, JE Lawn. Born Too Soon: The Global action report on preterm Birth. March of Dimes, PMNCH, Save the children, WHO. Available at: https://www.who.int/pmnch/media/news/2012/201204_borntoosoon-report.pdf.
4. Palazzi A, Nunes CC, Piccinini CA. Music therapy and musical stimulation in the context of prematurity: A narrative literature review from 2010–2015. J Clin Nurs. 2018; 27(1–2):1–20.
5. Cong X, Wu J, Vittner D, Xu W, Hussain N, Galvin S, et al. The Impact of Cumulative Pain/Stress on Neurobehavioral Development of Preterm Infants in the NICU. Early Hum Dev. 2017; 108: 1-21.
6. Dubois J, Benders M, Cachia A, Lazeyras F, Ha-Vinh Leuchter R, Sizonenko S V., et al. Mapping the Early Cortical Folding Process in the Preterm Newborn Brain. Cereb Cortex. 2008; 18(6):1444–1454.
7. Anderson DE, Patel AD. Infants born preterm, stress, and neurodevelopment in the neonatal intensive care unit: might music have an impact? Dev Med Child Neurol. 2018; 60(3):256–66.
8. Wight NE. Breastfeeding the NICU Infant. Clin Obstet Gynecol. 2015; 58(4):840–854.
9. Dewey KG. Symposium: Human Lactogenesis II: Mechanisms, Determinants and Consequences Maternal and Fetal Stress Are Associated with Impaired Lactogenesis in Humans 1. J. Nutr. 2001; 131(11):3012-3015.
10. Dobrzynska E, Cesarz H, Rymaszewska J. Music Therapy – History, definitions and application. Arch. Psychiatry Psychother. 2006; 8(1): 48-52.
11. Chorna OD, Slaughter JC, Wang L, Stark AR, Maitre NL, MacDonald N, et al. A pacifier-activated music player with mother’s voice improves oral feeding in preterm infants. Pediatrics. 2014; 133(3):462–468.
12. Yildiz A, Arikan D, Gözüm S, Taştekın A, Budancamanak İ. The Effect of the Odor of Breast Milk on the Time Needed for Transition From Gavage to Total Oral Feeding in Preterm Infants. J Nurs Scholarsh. 2011; 43(3).
13. Haslbeck FB. The interactive potential of creative music therapy with premature infants and their parents: A qualitative analysis. Nord J Music Ther. 2014;23(1):36–70.
14. O’Toole A, Francis K, Pugsley L. Does music positively impact preterm infant outcomes? Adv Neonatal Care. 2017; 17(3):192–202.
15. Pölkki T, Korhonen A. The effectiveness of music on pain among preterm infants in the neonatal intensive care unit: a systematic review. JBI Libr Syst Rev [Internet]. 2012; 10(58):4600–4609.
16. Mangat A, Oei J-L, Chen K, Quah-Smith I, Schmölzer G. A Review of Non-Pharmacological Treatments for Pain Management in Newborn Infants. Children. 2018; 5(10):130.
17. Cignacco E, Hamers JPH, Stoffel L, Lingen RA, Gessler P, McDougall J, et al. The efficacy of non-pharmacological interventions in the management of procedural pain in preterm and term neonates. Eur J Pain. 2007; 11(2):139–52.
18. Butt ML, Kisilevsky BS. Music modulates behaviour of premature infants following heel lance. Can J Nurs Res. 2000; 31(4):17–39.
19. Van der Heijden MJE, Oliai Araghi S, Jeekel J, Reiss IKM, Hunink MGM, van Dijk M. Do Hospitalized Premature Infants Benefit from Music Interventions? A Systematic Review of Randomized Controlled Trials. Thompson Coon J, editor. PLoS One [Internet]. 2016;11(9).
20. Caparros-Gonzalez RA, de la Torre-Luque A, Diaz-Piedra C, Vico FJ, Buela-Casal G. Listening to Relaxing Music Improves Physiological Responses in Premature Infants: A Randomized Controlled Trial. Adv Neonatal Care [Internet]. 2018; 18(1):58–69.
21. Bieleninik ucja, Ghetti C, Gold C. Music Therapy for Preterm Infants and Their Parents: A Meta-analysis. Pediatrics. 2016; 138(3):1–17.
22. Keith DR, Weaver BS, Vogel RL. The Effect of Music-Based Listening Interventions on the Volume, Fat Content, and Caloric Content of Breast Milk–Produced by Mothers of Premature and Critically Ill Infants. Adv Neonatal Care. 2012; 12(2):112–119.
23. Jayamala AK, Preethi BL, Pradeep GCM, Jaisri G. Impact of Music Therapy on Breast Milk Secretion in Mothers of Premature Newborns. J Clin Diagnostic Res. 2015; 9(4):CC4-CC6.
24. Yu J, Wells J, Wei Z, Fewtrell M. Randomized Trial Comparing the Physiological and Psychological Effects of Different Relaxation Interventions in Chinese Women Breastfeeding Their Healthy Term Infant. Breastfeed Med. 2018; 14(1):33–8.
25. Vianna MNS, Barbosa AP, Carvalhaes AS, Cunha AJLA. Music therapy may increase breastfeeding rates among mothers of premature newborns: a randomized controlled trial. J Pediatr (Rio J). 2011; 87(3):206–212.
Music Therapy and Musical Stimulation in Preterm Infants in Neonatal Intensive Care Units
Abstract
Every year, more than 15 million preterm infants are born of which a significant number is admitted to the Neonatal Intensive Care Unit. The combination of a critical period in neurocognitive development, parental
isolation and a hostile environment makes these patients particularly vulnerable to various cognitive, motor, linguistic, behavioral and socio-economic disabilities. Therefore, music therapy is proposed as a
non-invasive alternative to improve variables related to nutrition, pain and stress response, the physiological parameters of the newborn and breastfeeding.
Keywords: music, sound, preterm birth, neonatal intensive care unit, non-invasive, review.
- Introduction
A preterm infant is baby born before the 37th week of gestation (1). Every year, more than 15 million preterm infants are born, which amounts to 1 in 10 births. Despite technological improvements increasing the survival of these infants, the rate of preterm births is rising on a worldwide scale (2). Preterm birth can affect the cognitive, motor, linguistic, behavioral and socio-economic development of the infant, as well as the family’s mental health, especially that of the mother (3). A significant number of these infants requires intensive care to survive outside the intrauterine environment and, therefore, the Neonatal Intensive Care Unit (NICU) becomes the source of their first stimuli.
These units are characterized by parental isolation and the high number of invasive procedures (and thus painful and stressful) to which patients are subjected (4). These events occur during a period of early brain development, characterized by the formation of synaptic connections, the development of dendritic spines, axonal myelination and neocortical folding (5.6).
Several studies suggest the system of preterm infants possesses both the anatomical and neurochemical capabilities of pain perception (4), so those admitted to the NICU appear to be a particularly susceptible group for the potential disruption of these neurodevelopmental milestones. Furthermore, the stress response is activated by means of the hypothalamus-pituitary-adrenal axis and the sympathetic system, which determine physiological responses to the fight-or-flight response. These responses include an increase in heart and respiratory rates and an increase in cortisol. The implementation of these responses diverts energy resources from the forming nervous system (6).
- Preterm infant nutrition
In terms of feeding, it has been observed that music therapy (MT) helps preterm infants in the NICU to gradually substitute intravenous feeding with oral feeding. The use of a music player with songs sung by the mother significantly favors oral feeding. It was found that 94% of the infants stimulated with a music player with mother’s voice recordings were successfully fed orally at least 7 days earlier than those who were given a standard tranquilizer or listened to the mother’s voice only occasionally.
There were no significant differences regarding weight gain between the intervention and control groups. It should be noted that other studies suggest that oral stimulation has better results in improving oral feeding in preterm infants than the auditory stimulation (with lullabies). However, preterm infants who had auditory stimulation improved more than those in the control group, who had no intervention except for routine care (11). The differences between these groups were significant, finding that the group that received oral stimulation reached full oral feeding in a shorter period of time than those who received the auditory stimulation.
Finally, infants in the control group who had no intervention took longer to reach full oral feeding. Based on these data, differences in the suction capacity of the different groups were also found. This capacity was associated with the improvement of the oral feeding.
In some reviews, differences in the results obtained were considered depending on whether infants were exposed to live or recorded music. It is suggested that both types of MT improve the suction capacity of the premature infants and the time required to achieve full oral feeding (3). Other studies suggest that live music helps the premature infant to sleep more deeply than recorded music (12). The type of music also influences the amount of improvement. It has been observed that lullabies help improve oral feeding and increase the daily caloric intake of the infant. Additionally, the use of music players with songs sung by the mother significantly improves oral feeding when compared to other MS methods (13).
Figure 1 outlines the most representative findings of MT and MS on preterm neonatal nutrition.

- Pain and stress response
Preterm infants, mainly those who are admitted to the NICU, are usually in a stressful and over-stimulating environment during their hospital stay. Furthermore, they are exposed to numerous painful procedures, both diagnostic and therapeutic. All this has adverse consequences for their neurological development and pain perception system, as well as negative physiological alterations (6, 14-15). The negative effects of some analgesics, their misuse, and the (sometimes excessive) duration of their effects make non-pharmacological methods such as MT a widely used alternative (16).
Although many studies have been conducted on the effects of MT on newborns and preterm infants, these tend to focus on behavior and stimulation for development. Few studies investigate the response to pain (14) and stress, although some of them consider parameters related to both. In some randomized controlled trials, all referring to the newborn blood spot test, a decrease in respiratory rate (RR) and pain measured in the Neonatal Infant Pain Scale (NIPS) and Neonatal Facial Coding System (NFCS). An increase in transcutaneous partial pressure of oxygen (TcPO2) and significant effects on behavior were also observed. Infants older than 31 weeks benefited the most from this, especially right after the procedure (17). According to some authors, this could be due to their greater development, which allows for a better response to musical stimulation (14).
Regarding the type and form of application of the music, only recordings have been studied, these being classical music, intrauterine maternal pulse rates with relaxing music and lullabies, including Pacifier Activated Lullaby (PAL). Classical music had no significant positive results, nor did it managed to improve the benefits of breastfeeding. Likewise, PAL had no effect on pain, but on stress and behavior. Lullabies are recommended due to small variations in their melody, and so is live music. There are no comparable results for music volume, although some NICU recommendations on noise can be followed, such as not exceeding 45dB. It has also been suggested that joint implementation with other non-pharmacological methods, such as sucrose or non-nutritive sucking, could have greater positive effects than the application of MT alone, with the exception of breastfeeding (as mentioned above).
In conclusion, MT could have beneficial effects in the management of procedural pain in preterm infants in the NICU. However, there are very few studies on this subject, with little sample and very heterogeneous variables as to establish concrete practical indications to that effect. In relation to stress, although improvements in physiological parameters have been observed, it would be necessary to conduct further studies with objective measures of the activation of the hypothalamus-pituitary-adrenal axis (6).
- Physiological parameters
Several studies conducted in different parts of the world (including Spain), demonstrate the impact of MT on the physiological parameters of those born prematurely. In this section, multiple studies conducted with different sample sizes will be discussed. In the first case, MT produced beneficial physiological outcomes for 8 of the 12 preterm infants treated. After, individual evaluation, the following conclusions were drawn:
- In 3 cases, music is confirmed to improve short-term heart rate (HR) and oxygen saturation (SpO2).
- In 5 cases, classical music was used, Mozart being the most effective. The response to recordings of the mother’s voice was also evaluated, obtaining an improvement of SpO2 levels in 2 infants (13).
In the systematic review written by Van der Heijden et al. (18), 20 studies were reviewed, in which different categories of results were assessed. Of these, 14 evaluated the effect of MT and MS on HR, RF, SpO2 and cortisol levels. They found that in 7 of the 12 cases in which recorded music was used, there were no significant differences. Nevertheless, among the remaining cases, significant differences were observed. These were:
- An increase in SpO2.
- A decrease in HR and RR during and after MT.
Lastly, in four studies which measure the effect of live music, the reviewers concluded that significant differences could be observed in just two studies in terms of HR reduction.
Another study analyzed different parameters in newborns in two Spanish hospitals. Those parameters were measured before and after a 20-minute intervention of relaxing music three times a day, for three consecutive days. This study concluded that the use of relaxing music improves physiological parameters during hospitalization without any negative effects. The intervention group showed obtained improvement in HR and RR, with no significant changes in SpO2 and blood pressure (19). Similarly, various studies point to improvements in the physiological parameters of newborns treated with MT. One of these studies specifies that MT reduced infants’ RR by 3.91 breaths per minute. The result of HR was not significant – however, the authors attributed this result to the high volume of the recordings used (20).
In conclusion, all studies show an overall improvement of HR and RR, as well as an increase in SpO2 after MT and MS interventions in hospitalized newborns (3). Figure 1 shows the most relevant findings of this meta-analysis.
- Breastfeeding
Breastfeeding is beneficial for newborns as it provides them with all the nutrients they need during their first months of life. It contains the optimal amount of carbohydrates, proteins, fats, minerals, vitamins, digestive enzymes, hormones and antibodies. Thus, breastfeeding is important in preterm infants, as they are more immature due to a shorter gestation period and are at risk of suffering from different illnesses. Furthermore, preterm infants in the NICU require a higher quality nutritional intake than term infants. For this reason, their mothers need to be in the best conditions to breastfeed them. Nonetheless, mothers in the NICU experience high levels of stress and face physiological difficulties derived from an incomplete development of their breastfeeding mechanism. All this reduces the quality and quantity of the mother’s milk.
Health services should take measures to improve breastfeeding, such as the use of MT. This therapy helps reduce stress during breastfeeding sessions, improving the volume and fat content of breast milk. However, there is no evidence that it affects oxytocin levels (21).
On the other hand, it has been proved that MT lowers cortisol levels, which is a stress marker. It also decreases RR, arterial pressure, while changing fingertip temperature and perceived relaxation (22-23). Moreover, relaxation techniques that use images of the newborns improve the mother’s secretory activity, in addition to being a non-invasive procedure (21). MT constitutes one of the most accessible therapies as it can be being after discharge at a low cost. The choice of the music by the mothers, together with their involvement in music-based activities, has also revealed an improvement in milk production. At the same time, combining MT with yoga, progressive muscle relaxation, or guided imagery has given a better result in reducing maternal stress thus favorably affecting breastfeeding (21, 23-24).
In conclusion, as indicated in Figures 2 and 3 and Tables 1 and 2, breastfeeding provides physical and psychological benefits to both the mother and the infant (especially for preterms). Therefore, it is not only important to encourage breastfeeding through health education, but to provide activities and interventions like MT. This may help reduce maternal stress, improving the volume and quality of milk and strengthening the mother-child in such delicate situations as the newborn’s admission to the NICU.




- Conclusion
The purpose of this review was to examine the results published to date on MT and MS, and their impact on the health of preterm infants and breastfeeding in the NICU. Most studies and reviews seem to indicate that both MT and MS have positive effects on pain, stress, breastfeeding and physiological parameters. However, due to the great heterogeneity of interventions, methodology, data analysis and evaluation of the results, as well as the lack of a consistent and long-term follow-up, these results must be interpreted with caution. Likewise, it has been observed that MT and MS can be used together with other procedures and relaxation techniques. Future investigations may explore the efficiency of combined interventions. Regardless of the clinical significance of these therapies, their harmlessness and low cost make them an innovative strategy to improve the quality of infants admitted to the NICU infant and their families. Their admission of preterm infants to the NICU represents a critical situation that demands the best possible care and the most rigorous scientific work.
Conflicts of interest statement
The authors declare that there are no conflicts of interest in this article.
References
- Rellan Rodríguez S, García de Ribera C, Aragón García MP. El recién nacido prematuro. Madrid: Asociación Española de Pediatría; 2008 [Last accesed 15 March 2019]. Available at: http://www.aeped.es/sites/default/files/documentos/8_1.pdf
- P Howson, MV Kinney, JE Lawn. Born Too Soon: The Global action report on preterm Birth. March of Dimes, PMNCH, Save the children, WHO. Available at: https://www.who.int/pmnch/media/news/2012/201204_borntoosoon-report.pdf.
- Palazzi A, Nunes CC, Piccinini CA. Music therapy and musical stimulation in the context of prematurity: A narrative literature review from 2010–2015. J Clin Nurs. 2018; 27(1–2):1–20.
- Cong X, Wu J, Vittner D, Xu W, Hussain N, Galvin S, et al. The Impact of Cumulative Pain/Stress on Neurobehavioral Development of Preterm Infants in the NICU. Early Hum Dev. 2017; 108: 1-21.
- Dubois J, Benders M, Cachia A, Lazeyras F, Ha-Vinh Leuchter R, Sizonenko S V., et al. Mapping the Early Cortical Folding Process in the Preterm Newborn Brain. Cereb Cortex. 2008; 18(6):1444–1454.
- Anderson DE, Patel AD. Infants born preterm, stress, and neurodevelopment in the neonatal intensive care unit: might music have an impact? Dev Med Child Neurol. 2018; 60(3):256–66.
- Wight NE. Breastfeeding the NICU Infant. Clin Obstet Gynecol. 2015; 58(4):840–854.
- Dewey KG. Symposium: Human Lactogenesis II: Mechanisms, Determinants and Consequences Maternal and Fetal Stress Are Associated with Impaired Lactogenesis in Humans 1. J. Nutr. 2001; 131(11):3012-3015.
- Dobrzynska E, Cesarz H, Rymaszewska J. Music Therapy – History, definitions and application. Arch. Psychiatry Psychother. 2006; 8(1): 48-52.
- Chorna OD, Slaughter JC, Wang L, Stark AR, Maitre NL, MacDonald N, et al. A pacifier-activated music player with mother’s voice improves oral feeding in preterm infants. Pediatrics. 2014; 133(3):462–468.
- Yildiz A, Arikan D, Gözüm S, Taştekın A, Budancamanak İ. The Effect of the Odor of Breast Milk on the Time Needed for Transition From Gavage to Total Oral Feeding in Preterm Infants. J Nurs Scholarsh. 2011; 43(3).
- Haslbeck FB. The interactive potential of creative music therapy with premature infants and their parents: A qualitative analysis. Nord J Music Ther. 2014;23(1):36–70.
- O’Toole A, Francis K, Pugsley L. Does music positively impact preterm infant outcomes? Adv Neonatal Care. 2017; 17(3):192–202.
- Pölkki T, Korhonen A. The effectiveness of music on pain among preterm infants in the neonatal intensive care unit: a systematic review. JBI Libr Syst Rev [Internet]. 2012; 10(58):4600–4609.
- Mangat A, Oei J-L, Chen K, Quah-Smith I, Schmölzer G. A Review of Non-Pharmacological Treatments for Pain Management in Newborn Infants. Children. 2018; 5(10):130.
- Cignacco E, Hamers JPH, Stoffel L, Lingen RA, Gessler P, McDougall J, et al. The efficacy of non-pharmacological interventions in the management of procedural pain in preterm and term neonates. Eur J Pain. 2007; 11(2):139–52.
- Butt ML, Kisilevsky BS. Music modulates behaviour of premature infants following heel lance. Can J Nurs Res. 2000; 31(4):17–39.
- Van der Heijden MJE, Oliai Araghi S, Jeekel J, Reiss IKM, Hunink MGM, van Dijk M. Do Hospitalized Premature Infants Benefit from Music Interventions? A Systematic Review of Randomized Controlled Trials. Thompson Coon J, editor. PLoS One [Internet]. 2016;11(9).
- Caparros-Gonzalez RA, de la Torre-Luque A, Diaz-Piedra C, Vico FJ, Buela-Casal G. Listening to Relaxing Music Improves Physiological Responses in Premature Infants: A Randomized Controlled Trial. Adv Neonatal Care [Internet]. 2018; 18(1):58–69.
- Bieleninik ucja, Ghetti C, Gold C. Music Therapy for Preterm Infants and Their Parents: A Meta-analysis. Pediatrics. 2016; 138(3):1–17.
- Keith DR, Weaver BS, Vogel RL. The Effect of Music-Based Listening Interventions on the Volume, Fat Content, and Caloric Content of Breast Milk–Produced by Mothers of Premature and Critically Ill Infants. Adv Neonatal Care. 2012; 12(2):112–119.
- Jayamala AK, Preethi BL, Pradeep GCM, Jaisri G. Impact of Music Therapy on Breast Milk Secretion in Mothers of Premature Newborns. J Clin Diagnostic Res. 2015; 9(4):CC4-CC6.
- Yu J, Wells J, Wei Z, Fewtrell M. Randomized Trial Comparing the Physiological and Psychological Effects of Different Relaxation Interventions in Chinese Women Breastfeeding Their Healthy Term Infant. Breastfeed Med. 2018; 14(1):33–8.
- Vianna MNS, Barbosa AP, Carvalhaes AS, Cunha AJLA. Music therapy may increase breastfeeding rates among mothers of premature newborns: a randomized controlled trial. J Pediatr (Rio J). 2011; 87(3):206–212.
علاج الأطفال الخِدّج بالموسيقى والتحفيز الموسيقي في وحدات العناية المركزة لحديثي الولادة
AMU 2019. Volumen 1, Número 1
Fecha de envío: Fecha de aceptación: Fecha de publicación:
15/04/2019 22/04/2019 31/05/2019
Cita el artículo: Jiménez-Gutiérrez C, Pérez-del-Rincón M, Reduello-Guerrero P, Rodríguez-Rodríguez MP, Toral-López AM, Ureña-Paniego CA. Musicoterapia y estimulación musical en recién nacidos pretérmino en las unidades de cuidados intensivos neonatales. AMU. 2019; 1(1):8-29