Guillermo Ramírez-García 1; Pablo García-Molina 2; María Consuelo Flor-Cremades 3; Beatriz Muñoz-Rojas 4; Javier Moleón-Moya 5
1 Máster en Antropología y Genética Forense, Universidad de Granada (UGR)
2 Máster en Biotecnología, Universidad de Granada (UGR)
3 Facultad de Farmacia, Universidad de Granada (UGR)
4 Facultad de Medicina, Universidad de Granada (UGR)
5 Departamento de Farmacología, Facultad de Farmacia, Universidad de Granada (UGR)
Translated by:
Paula Asensi-Gómez 6; Ana Carbajo-García 7; Juan Luis Cobano-Jiménez 8; Elisa Lenker-Andrade 9; Iván Vázquez Delgado 9; Elena Vivas-del-Torno 6
6 Faculty of Human and Social Sciences, University of Comillas
7 Faculty of Human and Social Sciences, University Jaume I (UJI)
8 Faculty of Philosophy and Arts, University of Alcalá (UAH)
9 Faculty of Translation and Interpreting, University of Granada (UGR)
Resumen
Objetivos
El objetivo del trabajo fue evaluar el empleo de la hidroxicloroquina y el tocilizumab al comienzo de la pandemia, así como describir el perfil de los pacientes que recibieron estos tratamientos.
Métodos
Se analizaron las historias clínicas de 403 pacientes que ingresaron por COVID-19 desde el 1 de marzo hasta el 15 de abril de 2020 en el Hospital Universitario San Cecilio (Granada, España). Los datos recogidos incluían sexo, edad, días hospitalizados, patologías y/o tratamientos previos, posibles desenlaces y fármacos administrados en el centro. Para estimar las posibles asociaciones entre las variables definidas se utilizaron los parámetros estadísticos T de Student y χ² de Pearson.
Resultados
Los pacientes, con una edad media de 66 años (desviación estándar = 15,38), estuvieron hospitalizados un promedio de 15 días (desviación estándar = 12,89). La tasa de ingreso en UCI fue del 9,93 % y la de fallecimientos ascendió al 17,37 % del total de individuos. Durante la primera onda epidémica se administró la hidroxicloroquina a la mayoría de pacientes ingresados, mientras que el tocilizumab se restringió a los cuadros clínicos más graves.
Conclusiones
Los resultados obtenidos en este trabajo mostraron dos tendencias distintas en el uso de los fármacos estudiados. El tocilizumab se administró a un número muy reducido de pacientes, principalmente aquellos de mayor estancia o con complicaciones. La hidroxicloroquina se empleó independientemente de las características iniciales de los pacientes, con especial relevancia en aquellos que presentaban comorbilidades o estaban polimedicados.
Palabras clave: COVID-19, SARS-CoV-2, tocilizumab, hidroxicloroquina, hospitalización.
Keywords: COVID-19, SARS-CoV-2, tocilizumab, hydroxychloroquine, hospitalization
Introducción
En diciembre de 2019 se registró por primera vez en Wuhan (China) un caso de neumonía atípica de origen desconocido a la que posteriormente se bautizaría como Coronavirus disease 2019 (COVID-19). El agente etiológico de esta patología fue el coronavirus del síndrome respiratorio agudo severo (SARS-CoV-2), que ocasionó una pandemia mundial sin precedentes, con unas consecuencias devastadoras tanto para la salud pública como para la economía (1). El principal problema del SARS-CoV-2 fue la combinación de una propagación rápida junto con una sintomatología heterogénea que podía desembocar en la hospitalización o incluso la muerte (2). La mayoría de los pacientes diagnosticados de COVID-19 no revestían gravedad, siendo asintomáticos o presentando unos síntomas comunes inespecíficos tales como fiebre, tos y mialgia (3). Sin embargo, aquellos que desarrollaron complicaciones, como síndrome respiratorio agudo severo o infecciones, se asociaron a un mayor ingreso en la Unidad de Cuidados Intensivos (UCI) y elevada mortalidad (4). Con el objetivo de minimizar la morbimortalidad asociada a la COVID-19, el tratamiento farmacológico de las personas infectadas por SARS-CoV-2 se convirtió en una prioridad. Al inicio de la pandemia se ensayaron una miríada de agentes terapéuticos, intentando encontrar nuevas indicaciones para fármacos ya aprobados por organismos internacionales como la Food and Drug Administration o la European Medicines Agency, a la espera del desarrollo de una vacuna eficaz y segura (5).
En España, la primera onda epidémica abarcó desde comienzos de marzo hasta junio de 2020 (6). Los principales fármacos utilizados para tratar la enfermedad en hospitales y centros de atención primaria fueron principalmente antipalúdicos (hidroxicloroquina, HCQ), esteroides (metilprednisolona) y antivirales (remdesivir), acompañados por antibióticos en ciertos casos. Además, cabe mencionar el uso de los inhibidores de interleucina 1 (IL-1) o 6 (IL-6) como el tocilizumab (TCZ), e inhibidores selectivos de quinasas asociadas a Janus (JAK) como el ruxolitinib. También se emplearon varios tipos de interferón (IFN), como el IFN -1b. Por tanto, la tendencia durante este período fue el uso de agentes bastante inespecíficos, con la finalidad fundamental de evitar el deterioro de los órganos afectados, asociado con el progreso de la infección en los pacientes (7). La administración combinada de varios fármacos también fue una opción bastante utilizada, como la HCQ asociada con la azitromicina en pacientes con comorbilidades (8). Por otra parte, el uso de antivirales análogos a nucleósidos como el remdesivir se empleó en pacientes pertenecientes a grupos de riesgo, donde redujo la carga viral, aunque no mejoró considerablemente la sintomatología (9).
Entre los medicamentos que adquirieron una nueva indicación destacó la HCQ, un fármaco antimalárico y posteriormente usado en el lupus y la artritis (10). La evidencia sobre la que se sustentaba la indicación de este medicamento se basaba en su uso en los anteriores brotes de SARS-CoV-1 (11) y en la similitud de la COVID-19 con otras patologías inflamatorias. Inicialmente, tanto la HCQ como la cloroquina (CQ) se utilizaron principalmente en casos de mayor gravedad (12). Otro de los fármacos con más relevancia durante la pandemia fue el TCZ. En un primer momento, se evitó el uso de este medicamento por las incertidumbres planteadas en la literatura científica (13). Los estudios en los que se buscaba conocer la efectividad de dicho tratamiento frente a la COVID-19 no mostraban variaciones significativas con respecto a otras terapias (14,15). Sin embargo, conforme progresó la pandemia, se incrementó simultáneamente el número de individuos que recibieron el TCZ y el conocimiento sobre el mismo (16–18).
Ante esta situación, se planteó determinar el papel de estos dos fármacos durante la primera onda epidémica y su asociación con otras variables de interés. Por este motivo, el objetivo del estudio observacional longitudinal llevado a cabo fue evaluar el uso de la HCQ y el TCZ durante la primera etapa de la pandemia en España y, en última instancia, describir el perfil de los pacientes que recibieron estos tratamientos.
Materiales y métodos
Diseño
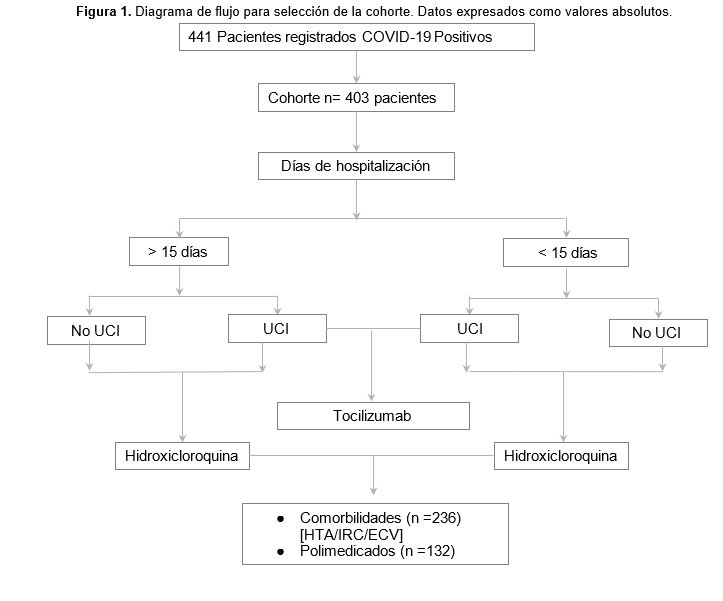
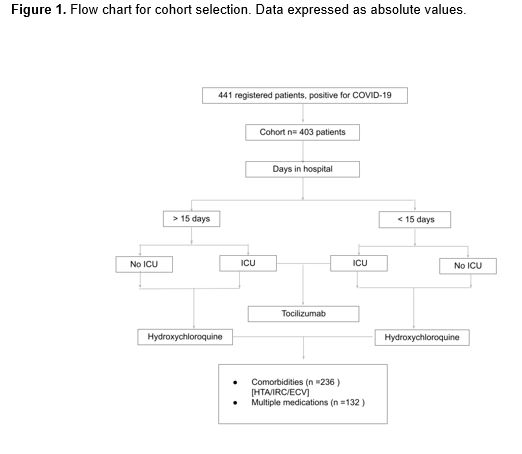
El planteamiento y desarrollo de este estudio observacional longitudinal se hizo bajo las recomendaciones de la guía Strengthening the Reporting of Observational studies in Epidemiology (STROBE). El análisis retrospectivo se llevó a cabo sobre los datos cedidos por el Hospital Universitario San Cecilio (Granada, España), y corresponden a 441 pacientes que fueron ingresados por COVID-19 en dicha instalación desde el 1 de marzo hasta el 15 de abril de 2020. A partir de la base de datos proporcionada se realizó un procedimiento de exclusión en el cual se descartaron aquellos individuos con un historial clínico incompleto, y se extrajo una muestra final de 403 pacientes. En el registro de variables se incluyeron tanto las características basales como los posibles desenlaces, así como los fármacos empleados en cada paciente (Figura 1).
Variables
Toda la información relativa a los pacientes se obtuvo a partir de los registros médicos electrónicos, donde se incluían las siguientes variables.
- Generalidades del paciente: edad, sexo y país de origen.
- Datos de hospitalización: fecha de entrada en el centro, fecha de alta o, en su defecto, defunción, rango de CURB65, comorbilidad, necesidad de ingreso en la UCI y número de días de hospitalización.
- Registros médicos de enfermedades previas: hipertensión (HTA), diabetes, patologías neumológicas, insuficiencia renal crónica (IRC), enfermedades cardiovasculares (ECV), enfermedades autoinmunes, neoplasias activas, asma y enfermedad pulmonar obstructiva crónica. También se incluyeron en este apartado los tratamientos vigentes asociados a las patologías de base, desde inmunosupresores a fármacos biológicos y polimedicación.
- Registro de la medicación administrada durante el periodo de hospitalización: HCQ, bolos de corticoides (CTC), lopinavir/ritonavir, azitromicina, inhibidores de enzima convertidora de angiotensina (IECA) o antagonistas de los receptores de angiotensina II (ARA2), antibióticos y TCZ. Además, se incluyó en este apartado la aparición de síndrome de liberación de citoquinas (SLC) o la candidatura a reanimación cardio-pulmonar (RCP) al momento del ingreso.
- Registros de dependencia y domiciliarias.
Análisis estadístico
El análisis estadístico de los datos se llevó a cabo mediante dos softwares de análisis, IBM SPSS ® (V.26) y R (R Foundation for Statistical Computing, Viena, Austria), V.4.0.4. Se evaluó la relación entre las variables anteriormente nombradas con los fármacos de interés mediante los parámetros estadísticos T de Student y χ² de Pearson, con un intervalo de confianza del 95 % en todos los análisis.
Consideraciones éticas
Este estudio fue aprobado por el Comité de Ética de la Investigación (CEI) provincial de Granada con fecha 1 de octubre de 2020. La base de datos empleada se utilizó de manera anonimizada, cumpliendo con la declaración de Helsinki.
Resultados
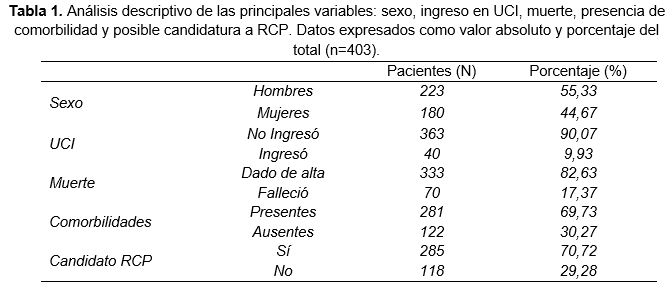
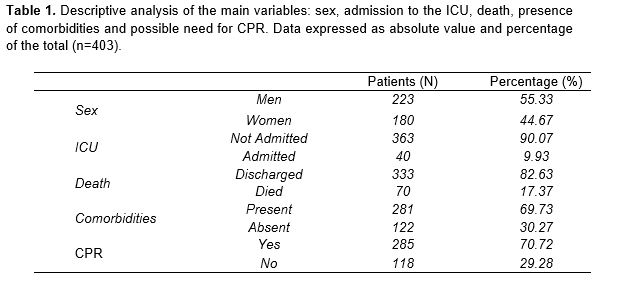
La población de estudio constaba de 403 individuos, de los cuales el 55,33 % eran varones y el 44,67 % mujeres. La edad media de los pacientes de la muestra fue de 66 años con una desviación estándar (SD) de 15,38. Por su parte, el promedio de hospitalización fue de 15 días (SD=12,89). Pese a la alta incidencia hospitalaria, solo fue precisa la derivación a UCI en 40 pacientes (9,9 % de los ingresados). De manera similar, un 17,4 % de la totalidad de sujetos tuvieron un desenlace fatal, lo que supone un valor de 70 defunciones. Cabe destacar que el 69,73 % de los pacientes presentaban alguna patología previa y 285 de los individuos totales fueron candidatos a RCP al momento del ingreso (Tabla 1).
Relación entre el tiempo de estancia en el hospital y el uso de un determinado fármaco
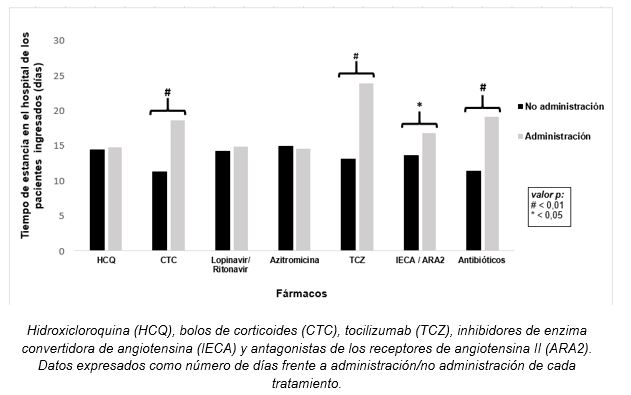
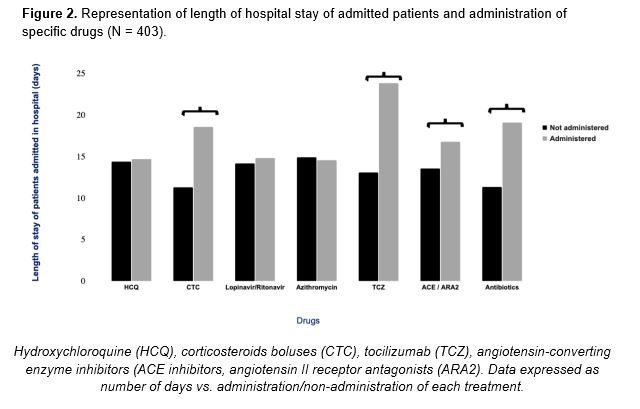
Antes de comenzar el análisis en profundidad de los fármacos de interés, se determinó la relación existente entre la administración de un determinado tratamiento y los días de hospitalización. Según los resultados obtenidos, la HCQ se empleó para un gran abanico de individuos, sin tener en cuenta los días de hospitalización. Por su parte, el TCZ, los CTC, los antibióticos y la combinación IECA/ARA2 fueron las opciones preferentes para aquellos pacientes que permanecieron durante mayor tiempo ingresados, tal y como se refleja en la Figura 2.
Figura 2. Representación del tiempo de estancia en el hospital de los pacientes ingresados y el suministro o no de un determinado fármaco (N = 403).
Tocilizumab
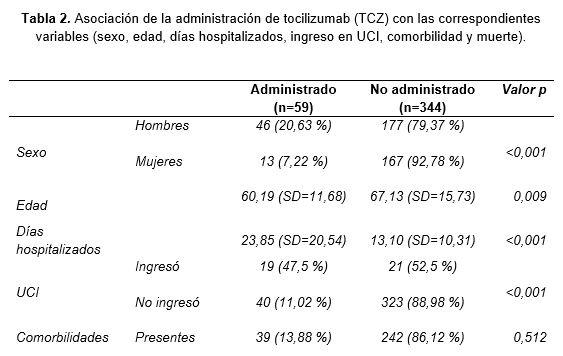
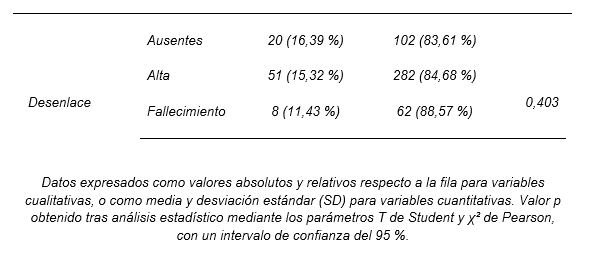
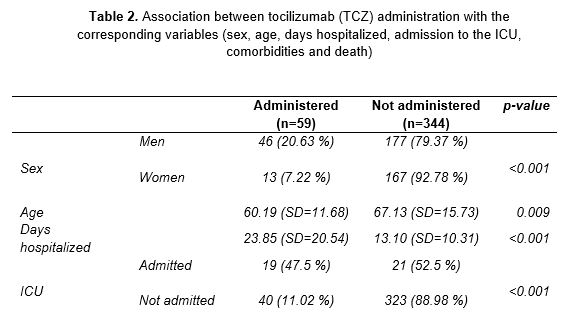
En relación al uso de TCZ (Tabla 2), se administró a 59 pacientes (14,6 % del total de sujetos), y se observó una asociación con su uso en varones (p<0,001). También se estableció una relación entre la utilización de TCZ y la edad (p=0,009), con un valor medio de 60 años (SD=11,68). Respecto al período de hospitalización, se observó que los pacientes en tratamiento con el fármaco permanecieron ingresados mayor tiempo que los que no lo recibieron (p<0,001). Complementariamente, se analizó el uso conjunto de TCZ con otros medicamentos de uso preferente en pacientes de larga estancia. Así pues, se observó una asociación en la coadministración del fármaco con antibióticos (p=0,006).
Puesto que una hospitalización prolongada podía relacionarse con el agravamiento de síntomas y la derivación a cuidados intensivos, se estudió la correlación entre el uso de TCZ y el ingreso en UCI. Conforme a lo esperado, se apreció una asociación entre la administración del fármaco y la necesidad de cuidados intensivos (p<0,001). En concordancia con lo anterior, se observó que la mayoría de pacientes tratados con TCZ fueron candidatos a RCP en el momento del ingreso hospitalario (p<0,001). De manera similar, 57 de los 59 individuos que recibieron el fármaco presentaron SLC eventualmente a lo largo de su estancia en el centro (p<0,001). Ante este hallazgo, se determinó la posible relación en el uso conjunto de TCZ y CTC y se encontró una fuerte asociación con un valor p<0,001.
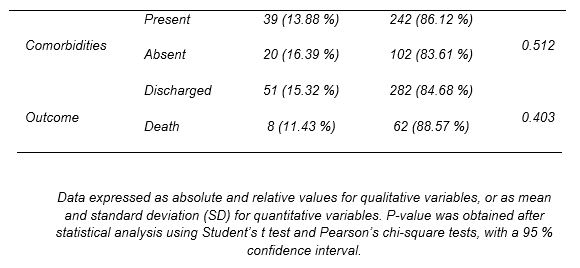
Finalmente, se analizaron otros factores de riesgo que podían estar implicados en el empeoramiento de la enfermedad. En contraste con los resultados previos, no se pudo relacionar el tratamiento con TCZ con la presencia de comorbilidades en el momento del ingreso en el centro (p=0,512). Tampoco se asoció el uso del TCZ con otros fármacos en pacientes polimedicados para patologías previas a la hospitalización (p=0,388).
Hidroxicloroquina
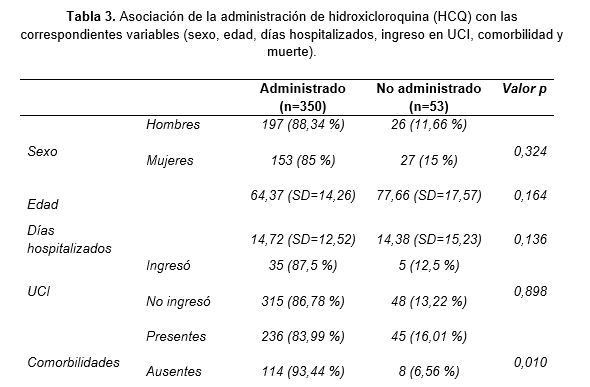
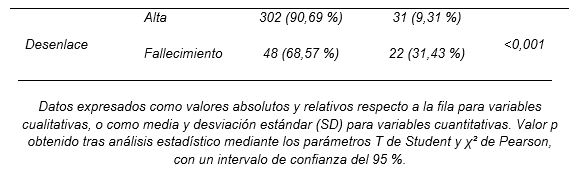
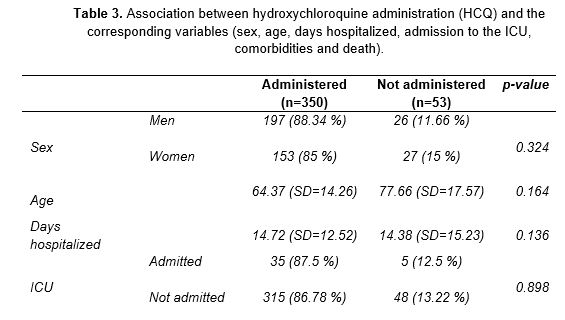
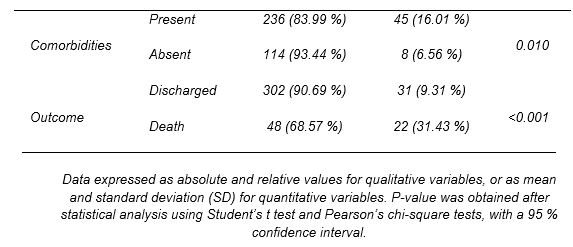
El otro fármaco objeto del estudio fue la HCQ, la cual se administró a 350 de los 403 individuos totales, lo que indica que el 86,8 % de pacientes ingresados por COVID-19 recibieron este tratamiento. Este grupo estaba conformado por 197 varones y 153 mujeres. El análisis estadístico no mostró ninguna asociación entre sexo y administración del fármaco (p=0,324), lo que indica que la HCQ se empleó de manera indiscriminada en ambos sexos (Tabla 3). Pese a su extenso uso, la HCQ no logró mejorar considerablemente el período de estancia en el centro (p=0,136). El promedio de días hospitalizados fue similar en ambos grupos, tanto el tratado como el no tratado con HCQ. Por su parte, aquellos individuos que ingresaron en la UCI fueron tratados con HCQ en una proporción similar a los que permanecieron en planta, y no se estableció una relación directa entre la derivación a cuidados intensivos y el uso del fármaco (p=0,898).
En contraposición a las variables anteriores, se encontró una asociación entre comorbilidad y administración de HCQ (p=0,01). Teniendo presente este hallazgo, se comprobó si el uso de HCQ estaba ligado a determinadas patologías previas que los pacientes padecían al ingresar en el hospital. Así pues, se observó una correlación entre los individuos a los que se administró el fármaco y que presentaban HTA (p=0,003), IRC (p=0,002) o ECV (p<0,001). En concordancia con esta tendencia, se apreció cómo aquellos sujetos que al momento del ingreso eran candidatos a RCP recibieron la HCQ en una proporción superior al resto (p<0,001). Los pacientes con comorbilidades necesitaron tratamientos específicos para sus patologías, por lo que se comprobó si la administración del fármaco estaba relacionada con la polimedicación y se obtuvo un valor p de 0,002.
Finalmente, se evaluó la correlación entre la HCQ y la utilización de otros agentes terapéuticos administrados en el hospital. Este análisis mostró una asociación en el uso combinado de HCQ con CTC (p=0,002), azitromicina (p<0,001) y lopinavir/ritonavir (p<0,001), los cuales se emplearon indistintamente del número de días de hospitalización.
Discusión
Relación entre el tiempo de estancia en el hospital y el uso de un determinado fármaco
En base a los resultados obtenidos, se observó que tanto el TCZ como los CTC, los IECA/ARA2 y los antibióticos se emplearon preferentemente en los pacientes con mayor período de hospitalización. La elección de estos fármacos se basó en la mejora de los síntomas. El TCZ es un agente que bloquea la unión de IL-6 con su receptor, lo que conlleva una disminución de los efectos de esta citoquina proinflamatoria (19). Por otra parte, los CTC, especialmente los glucocorticoides, se administraron debido a su capacidad de reducir el SLC de la COVID-19 en pacientes que manifiestan el síndrome hemofagocítico y de activación macrofágica (16). En cuanto al uso de IECA/ARA2, no existía uniformidad de criterio, ya que la interacción del SARS-CoV-2 con el sistema renina-angiotensina-aldosterona no estaba totalmente esclarecida. Por esa razón, aunque hubo autores detractores de la utilización de estos fármacos en la COVID-19 (20), la evidencia científica consideró que la terapia de la HTA era prioritaria (20,21). Por último, el tratamiento con antibióticos se reservó para aquellos individuos en los que aparecieron síntomas inespecíficos no asociados con la propia enfermedad o que presentaron complicaciones (22).
Tocilizumab
Los datos extraídos del análisis del TCZ mostraron una tendencia en el uso del fármaco en pacientes con una mayor estancia hospitalaria y una consecuente derivación a UCI. De hecho, se estableció una asociación relevante en el tratamiento combinado de TCZ con antibióticos. Estos agentes antimicrobianos se administraron en mayor medida a individuos hospitalizados durante períodos prolongados, de acuerdo con lo observado anteriormente (15).
En lo referente al uso de TCZ en UCI, se asoció el ingreso en cuidados intensivos con un agravamiento de la enfermedad. Esta descripción coincidió con lo publicado en otros estudios donde los pacientes que recibieron TCZ presentaban un estado peor de salud y vejez (23,24). La candidatura a RCP al momento del ingreso sirvió como indicador de aquellos sujetos con mayor riesgo de sufrir cuadros clínicos severos. El hecho de que el TCZ se utilizase preferentemente en este grupo de pacientes respaldó lo observado en la literatura previa (25).
Por otro lado, el TCZ se empleó casi exclusivamente para los individuos que presentaron SLC en cualquier momento durante su estancia hospitalaria. De acuerdo con estas observaciones, se encontró una asociación entre el uso del fármaco conjuntamente con CTC, los cuales se indicaron ampliamente para tratar esta complicación (16). Sin embargo, al evaluar la coadministración de TCZ con otros medicamentos en los pacientes estudiados no se pudo establecer ninguna correlación. La explicación de este resultado podría deberse al restringido uso del fármaco, ya que no existen evidencias de contraindicaciones en la utilización conjunta de TCZ y otros agentes terapéuticos (26, 27, 28).
Con toda la información obtenida del análisis se pudo describir de forma preliminar el paciente diana del TCZ en la cohorte estudiada. Los rasgos genéricos incluyeron una edad media de 60 años, una estancia en el hospital prolongada, asociada a ingreso en UCI y/o agravamiento de la enfermedad, y la aparición de SLC.
Hidroxicloroquina
Los resultados referidos a la HCQ mostraron un amplio uso del fármaco indistintamente de las características basales de los pacientes. Esta tendencia, comúnmente extendida durante el comienzo de la pandemia, se basó en recomendaciones que la posicionaban como una de las mejores elecciones frente al SARS-CoV-2 (29).
Atendiendo a las asociaciones más relevantes, se apreció una correlación entre la presencia de dos o más enfermedades al momento del ingreso y la indicación de HCQ. Al profundizar más en las patologías comprendidas dentro de las comorbilidades, se vio una asociación entre el fármaco y la HTA, ECV y ERC. De acuerdo con lo descrito por otros autores (30), tanto la HTA como las complicaciones derivadas de la misma, que constituyen la mayoría de ECV, requieren tratamientos crónicos. Por tanto, los pacientes con estas patologías están generalmente asociados a la polimedicación.
Se comprobó la relación entre los sujetos polimedicados y la administración de HCQ y se encontró una asociación relevante. La justificación de este resultado podría deberse en mayor medida al uso extendido del fármaco en la primera onda epidémica (12) que a los efectos protectores sobre este grupo de pacientes. No obstante, se observó una correlación entre la administración conjunta de HCQ y azitromicina, una combinación efectiva avalada por la evidencia científica del momento (31).
Los datos obtenidos del análisis permitieron esbozar el perfil de los pacientes que recibieron HCQ durante su período en el centro. Las características generales de estos sujetos fueron una edad media de 64 años, generalmente con presencia de enfermedades tales como HTA, IRC y/o ECV y, en menor proporción, polimedicados.
Limitaciones
Este estudio presenta ciertas limitaciones inherentes a su naturaleza observacional. Aparte de ellas, destacan el escaso tamaño muestral (n=403) obtenido tras los procedimientos de exclusión y el reducido período de recogida de datos. Aunque estas características podrían suponer un posible sesgo de imprecisión de cara a la generalización de los resultados, la robustez de los parámetros estadísticos empleados aumenta su validez (7).
Conclusiones
Los resultados mostraron dos tendencias totalmente distintas en el uso de los fármacos estudiados. Por un lado, el TCZ se administró a un número muy reducido de la totalidad de los sujetos. Se indicó principalmente en aquellos que permanecieron más días hospitalizados o cuyos cuadros clínicos se agravaron. También se asoció su uso a pacientes de UCI en coadministración con antibióticos. Por otro lado, la HCQ se impuso como uno de los agentes terapéuticos más empleados independientemente de las características iniciales de los pacientes. Adquirió especial relevancia en aquellos que presentaban comorbilidades y/o polimedicación. En los sujetos más graves se utilizó asociada a azitromicina.
Declaraciones
Agradecimientos
Los autores de este trabajo agradecen la implicación de los coordinadores y docentes de los cursos «Producción y traducción de artículos biomédicos (III ed.)» y «Traducción inversa de artículos científicos biomédicos (español-inglés)», así como al equipo de traducción al inglés de este artículo. De manera similar, los autores reconocen y agradecen la labor de los profesionales sanitarios que han trabajado durante la pandemia en el Hospital Universitario San Cecilio, por su inestimable trabajo y su admirable dedicación.
Conflictos de intereses
Los autores de este trabajo declaran no presentar ningún conflicto de interés.
Referencias
- Lemmon ME, Chapman I, Malcolm W, Kelley K, Shaw RJ, Milazzo A, et al. Beyond the First Wave: Consequences of COVID-19 on High-Risk Infants and Families. Am J Perinatol. 2020;37(12):1283.
- Awadasseid A, Wu Y, Tanaka Y, Zhang W. Initial success in the identification and management of the coronavirus disease 2019 (COVID-19) indicates human-to-human transmission in Wuhan, China. Int J Biol Sci. 2020;16(11):1846.
- Cheong J, Bartell N, Peeraphatdit T, Mosli M, Al-Judaibi B. Gastrointestinal and liver manifestations of COVID-19. Saudi J Gastroenterol Off J Saudi Gastroenterol Assoc. 2020;26(5):226.
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506.
- de Brouwer R, van Veldhuisen DJ, de Boer RA. Surviving the first COVID-19 wave and learning lessons for the second. Eur J Heart Fail. 2020.
- Gallego VM, Codorniu JM, Cabrero GR. The impact of COVID-19 on the elderly dependent population in Spain with special reference to the residential care sector. Ciência \& Saúde Coletiva. 2021;26:159–68.
- Gutiérrez-Abejón E, Tamayo E, Martin-Garcia D, Álvarez FJ, Herrera-Gómez F. Clinical Profile, Treatment and Predictors during the First COVID-19 Wave: A Population-Based Registry Analysis from Castile and Leon Hospitals. Int J Environ Res Public Health. 2020;17(24):9360.
- Risch HA. Early outpatient treatment of symptomatic, high-risk COVID-19 patients that should be ramped up immediately as key to the pandemic crisis. Am J Epidemiol. 2020;189(11):1218–26.
- Dubert M, Visseaux B, Isernia V, Bouadma L, Deconinck L, Patrier J, et al. Case report study of the first five COVID-19 patients treated with remdesivir in France. Int J Infect Dis. 2020;98:290–3.
- Bansal P, Goyal A, Cusick IV A, Lahan S, Dhaliwal HS, Bhyan P, et al. Hydroxychloroquine: A comprehensive review and its controversial role in coronavirus disease 2019. Ann Med. 2021;53(1):117–34.
- Ibáñez S, Martinez O, Valenzuela F, Silva F, Valenzuela O. Hydroxychloroquine and chloroquine in COVID-19: should they be used as standard therapy? Clin Rheumatol. 2020;39:2461–5.
- Pereira BB. Challenges and cares to promote rational use of chloroquine and hydroxychloroquine in the management of coronavirus disease 2019 (COVID-19) pandemic: a timely review. J Toxicol Environ Heal Part B. 2020;23(4):177–81.
- Russell CD, Millar JE, Baillie JK. Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury. Lancet. 2020;395(10223):473–5.
- Sciascia S, Aprà F, Baffa A, Baldovino S, Boaro D, Boero R, et al. Pilot prospective open, single-arm multicentre study on off-label use of tocilizumab in severe patients with COVID-19. Clin Exp Rheumatol. 2020;38(3):529–32.
- Campochiaro C, Della-Torre E, Cavalli G, De Luca G, Ripa M, Boffini N, et al. Efficacy and safety of tocilizumab in severe COVID-19 patients: a single-centre retrospective cohort study. Eur J Intern Med. 2020;76:43–9.
- Rubio JLC, Del Castillo J de DL, de la Hera Fernández J, Arrabal EG, Ruiz MC, Centeno NO. Effectiveness of corticoid pulses in patients with cytokine storm syndrome induced by SARS-CoV-2 infection. Med Clínica (English Ed. 2020;155(4):159–61.
- Capra R, De Rossi N, Mattioli F, Romanelli G, Scarpazza C, Sormani MP, et al. Impact of low dose tocilizumab on mortality rate in patients with COVID-19 related pneumonia. Eur J Intern Med. 2020;76:31–5.
- Stone JH, Frigault MJ, Serling-Boyd NJ, Fernandes AD, Harvey L, Foulkes AS, et al. Efficacy of tocilizumab in patients hospitalized with Covid-19. N Engl J Med. 2020;383(24):2333–44.
- Luo P, Liu Y, Qiu L, Liu X, Liu D, Li J. Tocilizumab treatment in COVID-19: a single center experience. J Med Virol. 2020;92(7):814–8.
- Arcos FS, Puche AR, Vera TV. Controversy regarding ACE inhibitors/ARBs in Covid-19. Rev Esp Cardiol (Engl Ed). 2020;73(6):516.
- Schiffrin EL, Flack JM, Ito S, Muntner P, Webb RC. Hypertension and COVID-19. Oxford University Press US; 2020.
- Miranda C, Silva V, Capita R, Alonso-Calleja C, Igrejas G, Poeta P. Implications of antibiotics use during the COVID-19 pandemic: present and future. J Antimicrob Chemother. 2020;75(12):3413–6.
- Klopfenstein T, Zayet S, Lohse A, Balblanc J-C, Badie J, Royer P-Y, et al. Tocilizumab therapy reduced intensive care unit admissions and/or mortality in COVID-19 patients. Med Mal Infect. 2020;50(5):397–400.
- Gupta S, Wang W, Hayek SS, Chan L, Mathews KS, Melamed ML, et al. Association between early treatment with tocilizumab and mortality among critically ill patients with COVID-19. JAMA Intern Med. 2021;181(1):41–51.
- Colaneri M, Bogliolo L, Valsecchi P, Sacchi P, Zuccaro V, Brandolino F, et al. Tocilizumab for treatment of severe COVID-19 patients: preliminary results from SMAtteo COvid19 REgistry (SMACORE). Microorganisms. 2020;8(5):695.
- Samaee H, Mohsenzadegan M, Ala S, Maroufi SS, Moradimajd P. Tocilizumab for treatment patients with COVID-19: Recommended medication for novel disease. Int Immunopharmacol. 2020;107018.
- Xu X, Han M, Li T, Sun W, Wang D, Fu B, et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc Natl Acad Sci. 2020;117(20):10970–5.
- Fontana F, Alfano G, Mori G, Amurri A, Tei L, Ballestri M, et al. Covid-19 pneumonia in a kidney transplant recipient successfully treated with tocilizumab and hydroxychloroquine. Am J Transplant. 2020;20(7):1902–6.
- Zhou D, Dai S-M, Tong Q. COVID-19: a recommendation to examine the effect of hydroxychloroquine in preventing infection and progression. J Antimicrob Chemother. 2020;75(7):1667–70.
- Fravel MA, Ernst M. Drug Interactions with Antihypertensives. Curr Hypertens Rep. 2021;23(3):1–8.
- Gautret P, Lagier J-C, Parola P, Meddeb L, Mailhe M, Doudier B, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. Int J Antimicrob Agents. 2020;56(1):105949.
Hydroxychloroquine and Tocilizumab in the Treatment of COVID-19: A Longitudinal Observational Study
Abstract
Objectives
The objective of this study is to evaluate the use of hydroxychloroquine and tocilizumab at the beginning of the COVID-19 pandemic and to describe the profile of patients who received these treatments.
Method
The medical records of 403 patients admitted for COVID-19 from March 1 to April 15, 2020 at the San Cecilio University Hospital (Granada, Spain) were analyzed. The data collected included sex, age, days hospitalized, previous pathologies and/or treatments, possible outcomes and drugs administered at the hospital. Student’s t-test and Pearson’s chi-square tests were used as statistical parameters to estimate the possible associations between the defined variables.
Results
Patients with a mean age of 66 years (standard deviation = 15.38), were hospitalized for an average of 15 days (standard deviation = 12.89). The ICU admission rate was 9.93 %, and the death rate added up to 17.37 % of the total number of patients. During the first wave of the pandemic, hydroxychloroquine was administered to the majority of hospitalized patients, while tocilizumab was restricted to the more severe cases.
Conclusions
The results showed two distinct trends in the use of the drugs studied. Tocilizumab was administered to a small number of patients, mainly those with longer length of stay or with complications. Hydroxychloroquine was administered independently of the initial characteristics of patients, especially those who presented comorbidities or took multiple medications.
Keywords: COVID-19, SARS-CoV-2, tocilizumab, hydroxychloroquine, hospitalization
Introduction
In December 2019, a case of atypical pneumonia of unknown origin was reported for the first time in Wuhan (China), which was later named as coronavirus disease 19 (COVID-19). The etiological agent of this pathology is the coronavirus responsible for the severe acute respiratory syndrome (SARS-CoV-2), which caused an unprecedented global pandemic with devastating consequences not only for public health, but for the economy (1). The main problem with SARS-CoV-2 was the combination of rapid spread and heterogeneous symptomatology that could lead to hospitalization or even death (2). Most patients diagnosed with COVID-19 were not severe cases, being asymptomatic or having common nonspecific symptoms such as fever, cough and myalgia (3). Nevertheless, those who developed complications like severe acute respiratory syndrome or infections were associated with increased admission to the ICU and high mortality (4). To reduce the morbidity and mortality rates associated with COVID-19, pharmacological treatment of patients infected with SARS-CoV-2 became a priority. At the beginning of the pandemic, a large number of therapeutic agents were tested in search of new indications for drugs already approved by international organisations, such as the Food and Drug Administration (FDA) or the European Medicines Agency (EMA), while awaiting the development of an effective and safe vaccine (5).
In Spain, the first wave of the pandemic lasted from the beginning of March until June 2020 (6). The main drugs used to treat the disease in hospitals and primary care centers were antimalarial medication (hydroxychloroquine [HCQ]), steroids (methylprednisolone) and antivirals (remdesivir), together with antibiotics in some cases. The use of interleukin 1 (IL-1) or 6 (IL-6) inhibitors, such as tocilizumab (TCZ), and Janus kinase inhibitors, such as ruxolitinib, is also worth mentioning. Several types of interferon (IFN), such as IFN-1b, were also used. Therefore, the trend during this period was the use of rather nonspecific agents, with the aim of avoiding the deterioration of the affected organs associated with the progression of the infection in patients (7). The combined administration of several drugs was also widely used, such as HCQ coupled with azithromycin in patients with comorbidities (8). In addition, nucleoside analogue antivirals, such as remdesivir, were used in high-risk groups. This reduced the viral load, but it did not considerably improve symptomatology (9).
Among the drugs with a new indication was HCQ stood out, an antimalarial drug also used to treat lupus and arthritis. The evidence supporting the indication for this drug was based on its used in previous SARS-CoV-1 outbreaks (11) and on the similarity of COVID-19 to other inflammatory pathologies. Initially, both HCQ and chloroquine (CQ) were mostly used in more severe cases (12). Another relevant drug during the pandemic was TCZ. At first, its used was avoided due to the uncertainties raised in the scientific literature (13). The studies that sought to determine the effectiveness of this drug against COVID-19 did not show significant variations with respect to other treatments (14, 15). However, as the pandemic progressed, the number of individuals receiving TCZ and the knowledge of this drug increased simultaneously (16-18).
As such, we set out to determine the role of these two drugs during the first wave of the pandemic and their association with other variables of interest. The objective of this longitudinal observational study was to evaluate the use of HCQ and TCZ during this period in Spain and ultimately to describe the profile of the patients who received these treatments.
Materials and methods
Design
The planning and development of this longitudinal observational study was made following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. The retrospective analysis was carried out on data provided by the San Cecilio University Hospital (Granada, Spain) and corresponds to 441 patients hospitalized for COVID-19 in this facility from March 1 to April 15, 2020. From the database provided, individuals with an incomplete medical history were discarded, resulting in a final sample of 403 patients. The registry of variables included baseline characteristics and possible outcomes, as well as drugs used for each patient (Figure 1).
Variables
All patient-related information was obtained from electronic medical records where the following variables were included:
- Patient’s general information: age, sex and country of origin.
- Hospitalization data: date of admission date to the center; date of discharge from the center or, otherwise, date of death; CURB-65 score; comorbidity; need for admission to the ICU and number of days hospitaliz
- Medical records of previous diseases: hypertension (HT), diabetes (DM), pneumological pathologies, chronic kidney failure (CKF), cardiovascular diseases (CVD), autoimmune diseases, neoplasms, asthma and chronic obstructive pulmonary disease (COPD). Also included in this section were current treatments associated with underlying pathologies, going from immunosuppressants to biologic drugs, as well as polypharmacy.
- Records of medication administered during hospitalization: HCQ, corticosteroids boluses (CTC), lopinavir/ritonavir, azithromycin, angiotensin-converting enzyme inhibitors (ACE inhibitors) or angiotensin II receptor antagonists (ARA2), antibiotics and TCZ. This section also included if the occurrence of cytokine release syndrome (CRS) or the need for cardiopulmonary resuscitation (CPR) when admitted to the hospital.
- Dependency and domiciliary records.
Statistical analysis
The statistical analysis of the data was made using two analysis software packages: IBM SPSS ® (V.26) and R (R Foundation for Statistical Computing, Wien, Austria), V.4.0.4. The relationship between the variables previously mentioned and the drugs of interest was evaluated using the following statistical parameters: Student’s t-tests and Pearson’s chi-square tests, with a 95 % confidence interval in all the analyses.
Ethical considerations
The provincial Research Ethics Committee of Granada approved this study on October 1, 2020. The database used was anonymized, in compliance with the Declaration of Helsinki.
Results
The study population consisted of 403 individuals, of whom 55.33 % were male and 44.67 % female. The mean age of the patients in the sample was 66 years, with a standard deviation (SD) of 15.38. The average length of hospitalization was 15 days (SD=12.89). Despite the high incidence of hospitalization, only 40 patients (9.9 %) required admission to the ICU. Similarly, only 17.4 % of the subjects had a fatal outcome, amounting to 70 deaths. It should be noted that 69.73 % of the patients had some previous pathology, and 285 of the total number of patients required CPR at the time of admission (Table 1).
Relationship between length of hospital stay and use of a given drug
Before starting the in-depth analysis of the drugs under study, the relationship between the administration of a given drug and the number of days of hospitalization was determined. According to the results obtained, HCQ was used for a wide range of individuals, regardless of the number of days of hospitalization. In turn, TCZ, CTC, antibiotics and the ACE inhibitors/ARA2 combination were the preferred options for those patients who remained longer in hospital, as shown in Figure 2.
Tocilizumab
TCZ (Table 2) was administered to 59 patients (14.6 % of the total number of subjects). Data suggests an association with its use in men (p<0.001). A relationship was also established between TCZ use and age (p=0.009), with a mean value of 60 years (SD=11.68). Regarding the hospitalization period, patients treated with this drug remained hospitalized longer than those who did not receive it (p<0.001). In addition, the joint use of TCZ with other drugs of preferential use in long-stay patients was analyzed. As a result, an association was observed in the coadministration of the drug with antibiotics (p=0.006).
Since prolonged hospitalization could be related to the worsening of symptoms and the referral to intensive care, the correlation between the use of TCZ and admission to the ICU was studied. As expected, there was an association between drug administration and the need for intensive care (p<0.001). The majority of patients treated with TCZ required CPR at the time of admission (p<0.001). Similarly, 57 of the 59 patients who received the drug eventually presented CRS during hospitalization (p<0.001). Considering this finding, a relation in the joint use of TCZ and CTC was determined, with a p-value of <0.001.
Finally, other risk factors that could be involved in the worsening of the disease were analyzed. In contrast to previous results, it was not possible to relate TCZ use with the presence of comorbidities at the time admission to the hospital (p=0.512), nor was it associated with other drugs in patients taking multiple medications prior hospitalization (p=0.388).
Hydroxychloroquine
The other drug under study was HCQ. It was administered to 350 out of the 403 patients, that is, 86.8% of the patients admitted for COVID-19. This group comprised 197 males and 153 females. The statistical analysis performed found no association between sex and drug administration (p=0.324), showing that HCQ was used irrespective of sex (Table 3). Despite its extensive use, HCQ failed to significantly reduce the length of hospital stay (p=0.136). The average number of days hospitalized was similar in those treated and not treated with HCQ. In addition, those who were eventually admitted to the ICU were treated with HCQ in a similar proportion to those who remained on the ward. No direct association was established between referral to intensive care and the use of this drug (p=0.898).
Unlike the previous variables, an association was found between comorbidity and HCQ use (p=0.01). Considering this finding, the relationship between HCQ use and patients with previous at the time of admission to the hospital was also tested. A correlation was observed between individuals who received the drug and who presented HT (p=0.003), CKF (p=0.002) or CVD (p<0.001). Accordingly, patients who needed CPR at the time of admission received HCQ in a higher proportion than the rest of patients (p<0.001). Patients with comorbidities required specific treatments for their pathologies. Therefore, the relationship between drug administration and multiple medications was tested, with a p-value of 0.002.
Finally, the correlation between HCQ and the use of other therapeutic agents administered in the hospital was analyzed. An association was found between in the joint use of HCQ and CTC (p=0.002), azithromycin (p<0.001) and lopinavir/ritonavir (p<0.001), which were used regardless of the number of days of hospitalization.
Discussion
Relationship between length of hospital stay and use of a given drug
Based on the results, it was observed that TCZ, CTCs, ACE /ARA2 inhibitors and antibiotics were preferentially used in patients with a longer hospital stay. The choice of these drugs was based on the improvement of symtoms. TCZ is an agent that blocks the binding of IL-6 to its receptor, leading to a decrease in the effects of this proinflammatory cytokine (19). CTCs, especially glucocorticoids, were also administered due to their ability to reduce the CRS associated with COVID-19 in patients who manifest hemophagocytic syndrome (HPS) and macrophage activation syndrome (MAS) (16). Regarding the use of ACE/ARA2 inhibitors, there were no standardized criteria, as the interaction of SARS-CoV-2 with the Renin-Angiotensin-Aldosterone system was not fully clear. For this reason, although some authors rejected the use of these drugs in COVID-19 patients (20), scientific evidence proofs HT treatment a priority (20, 21). Finally, antibiotic treatment was reserved for patients who presented nonspecific symptoms not associated with the disease or patients with complications (22).
Tocilizumab
The data obtained from analysing TCZ showed a trend in the use of this drug in patients with a longer hospital stay and consequent referral to the ICU. In fact, a relevant association was found in the joint use of TCZ and antibiotics. These antimicrobial agents were administered to a greater extent to individuals hospitalized for extended periods, as observed previously (15).
Regarding the use of TCZ in the ICU, admission to intensive care was associated with a worsening of the disease. This description matched the findings of other studies in which patients who received TCZ presented poorer health and old age (23,24). Requiring CPR at admission served as an indicator of patients at higher risk of severe COVID-19. The fact that TCZ was preferentially used for this group of patients supports what was observed in previous studies (25).
In addition, TCZ was used almost exclusively for individuals who presented CRS at any time during hospitalization. Given this information, an association was found between the use of the drug in conjunction with CTC, which were widely indicated to treat this complication (16). However, when evaluating the coadministration of TCZ with other drugs in the patients under study, no correlation could be established. The explanation for this could be owed to the restricted use of the drug, as there is no evidence of contraindications in the joint use of TCZ and other therapeutic agents (26, 27, 28).
With all the information obtained from the analysis, it was possible to preliminarily describe the TCZ target patient in the cohort studied. Generic features included a mean age of 60 years, extended hospital stay associated with ICU admission or worsening of the disease, and the occurrence of CRS.
Hydroxychloroquine
The results regarding HCQ showed a wide use of the drug regardless of the baseline characteristics of the patients. This trend was common during the beginning of the pandemic and was based on recommendations that positioned it as one of the best choices against SARS-CoV-2 (29).
Regarding the most relevant associations, a correlation was observed between the presence of two or more diseases at the time of admission and the indication for HCQ. When examining the pathologies included among comorbidities, an association was found between the drug and HT, CVD and CKD. As described by other authors (30), both HT and the complications derived from it, which constitute the majority of CVD cases, require chronic treatment. Therefore, patients with these pathologies generally receive multiple medications.
The relationship between subjects receiving multiple medications and the administration of HCQ was tested and a relevant association was found. The reason for this result could be the widespread use of the drug during the first wave of the pandemic (12) rather than the protective effects on this group of patients. Nonetheless, a correlation was observed between the joint administration of HCQ and azithromycin, an effective combination supported by scientific evidence (31).
The data obtained from the analysis enables the profiling of patients who received HCQ during hospitalization. The general characteristics of these subjects were: a mean age of 64 years, generally presenting pathologies such as HT, CKD and CVD, and, to a lesser extent, patients receiving multiple medications.
Limitations
The study has certain limitations inherent to its observational nature. Other than these, the small sample size (n=403) due to exclusion criteria and the short period of data collection are worth noting. Although these characteristics could imply a possible imprecision bias with regard to the generalization of the results, the strength of the statistical parameters used increases their validity (7).
Conclusions
The results showed two totally different trends in the use of the drugs under study. On the one hand, TCZ was administered to a very small number of the total number of subjects. It was mainly indicated for those who remained hospitalized longer or whose clinical conditions worsened. Its use was also associated with ICU patients in coadministration with antibiotics. On the other hand, HCQ became one of the most widely used therapeutic agents regardless of the initial characteristics of the patients. It became particularly relevant for patients with comorbidities or receiving multiple medications. In most severe cases, HCQ was used in conjunction with azithromycin.
Statements
Acknowledgements
The authors of this paper would like to thank the involvement of the coordinating and teaching staff of the “Producción y traducción de artículos científicos biomédicos (III ed.)” and the “Traducción inversa de artículos científicos biomédicos (español-inglés)” courses, as well as the English translation team. Likewise, the authors acknowledge and thank the healthcare professionals who worked during the pandemic at the Hospital Universitario San Cecilio (Granada) for their invaluable work and admirable commitment.
Conflicts of interest
The authors of this paper declare no conflicts of interest.
References
- Lemmon ME, Chapman I, Malcolm W, Kelley K, Shaw RJ, Milazzo A, et al. Beyond the First Wave: Consequences of COVID-19 on High-Risk Infants and Families. Am J Perinatol. 2020;37(12):1283.
- Awadasseid A, Wu Y, Tanaka Y, Zhang W. Initial success in the identification and management of the coronavirus disease 2019 (COVID-19) indicates human-to-human transmission in Wuhan, China. Int J Biol Sci. 2020;16(11):1846.
- Cheong J, Bartell N, Peeraphatdit T, Mosli M, Al-Judaibi B. Gastrointestinal and liver manifestations of COVID-19. Saudi J Gastroenterol Off J Saudi Gastroenterol Assoc. 2020;26(5):226.
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506.
- de Brouwer R, van Veldhuisen DJ, de Boer RA. Surviving the first COVID-19 wave and learning lessons for the second. Eur J Heart Fail. 2020.
- Gallego VM, Codorniu JM, Cabrero GR. The impact of COVID-19 on the elderly dependent population in Spain with special reference to the residential care sector. Ciência & Saúde Coletiva. 2021;26:159–68.
- Gutiérrez-Abejón E, Tamayo E, Martin-Garcia D, Álvarez FJ, Herrera-Gómez F. Clinical Profile, Treatment and Predictors during the First COVID-19 Wave: A Population-Based Registry Analysis from Castile and Leon Hospitals. Int J Environ Res Public Health. 2020;17(24):9360.
- Risch HA. Early outpatient treatment of symptomatic, high-risk COVID-19 patients that should be ramped up immediately as key to the pandemic crisis. Am J Epidemiol. 2020;189(11):1218–26.
- Dubert M, Visseaux B, Isernia V, Bouadma L, Deconinck L, Patrier J, et al. Case report study of the first five COVID-19 patients treated with remdesivir in France. Int J Infect Dis. 2020;98:290–3.
- Bansal P, Goyal A, Cusick IV A, Lahan S, Dhaliwal HS, Bhyan P, et al. Hydroxychloroquine: A comprehensive review and its controversial role in coronavirus disease 2019. Ann Med. 2021;53(1):117–34.
- Ibáñez S, Martinez O, Valenzuela F, Silva F, Valenzuela O. Hydroxychloroquine and chloroquine in COVID-19: should they be used as standard therapy? Clin Rheumatol. 2020;39:2461–5.
- Pereira BB. Challenges and cares to promote rational use of chloroquine and hydroxychloroquine in the management of coronavirus disease 2019 (COVID-19) pandemic: a timely review. J Toxicol Environ Heal Part B. 2020;23(4):177–81.
- Russell CD, Millar JE, Baillie JK. Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury. Lancet. 2020;395(10223):473–5.
- Sciascia S, Aprà F, Baffa A, Baldovino S, Boaro D, Boero R, et al. Pilot prospective open, single-arm multicentre study on off-label use of tocilizumab in severe patients with COVID-19. Clin Exp Rheumatol. 2020;38(3):529–32.
- Campochiaro C, Della-Torre E, Cavalli G, De Luca G, Ripa M, Boffini N, et al. Efficacy and safety of tocilizumab in severe COVID-19 patients: a single-centre retrospective cohort study. Eur J Intern Med. 2020;76:43–9.
- Rubio JLC, Del Castillo J de DL, de la Hera Fernández J, Arrabal EG, Ruiz MC, Centeno NO. Effectiveness of corticoid pulses in patients with cytokine storm syndrome induced by SARS-CoV-2 infection. Med Clínica (English Ed. 2020;155(4):159–61.
- Capra R, De Rossi N, Mattioli F, Romanelli G, Scarpazza C, Sormani MP, et al. Impact of low dose tocilizumab on mortality rate in patients with COVID-19 related pneumonia. Eur J Intern Med. 2020;76:31–5.
- Stone JH, Frigault MJ, Serling-Boyd NJ, Fernandes AD, Harvey L, Foulkes AS, et al. Efficacy of tocilizumab in patients hospitalized with Covid-19. N Engl J Med. 2020;383(24):2333–44.
- Luo P, Liu Y, Qiu L, Liu X, Liu D, Li J. Tocilizumab treatment in COVID-19: a single center experience. J Med Virol. 2020;92(7):814–8.
- Arcos FS, Puche AR, Vera TV. Controversy regarding ACE inhibitors/ARBs in Covid-19. Rev Esp Cardiol (Engl Ed). 2020;73(6):516.
- Schiffrin EL, Flack JM, Ito S, Muntner P, Webb RC. Hypertension and COVID-19. Oxford University Press US; 2020.
- Miranda C, Silva V, Capita R, Alonso-Calleja C, Igrejas G, Poeta P. Implications of antibiotics use during the COVID-19 pandemic: present and future. J Antimicrob Chemother. 2020;75(12):3413–6.
- Klopfenstein T, Zayet S, Lohse A, Balblanc J-C, Badie J, Royer P-Y, et al. Tocilizumab therapy reduced intensive care unit admissions and/or mortality in COVID-19 patients. Med Mal Infect. 2020;50(5):397–400.
- Gupta S, Wang W, Hayek SS, Chan L, Mathews KS, Melamed ML, et al. Association between early treatment with tocilizumab and mortality among critically ill patients with COVID-19. JAMA Intern Med. 2021;181(1):41–51.
- Colaneri M, Bogliolo L, Valsecchi P, Sacchi P, Zuccaro V, Brandolino F, et al. Tocilizumab for treatment of severe COVID-19 patients: preliminary results from SMAtteo COvid19 REgistry (SMACORE). Microorganisms. 2020;8(5):695.
- Samaee H, Mohsenzadegan M, Ala S, Maroufi SS, Moradimajd P. Tocilizumab for treatment patients with COVID-19: Recommended medication for novel disease. Int Immunopharmacol. 2020;107018.
- Xu X, Han M, Li T, Sun W, Wang D, Fu B, et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc Natl Acad Sci. 2020;117(20):10970–5.
- Fontana F, Alfano G, Mori G, Amurri A, Tei L, Ballestri M, et al. Covid-19 pneumonia in a kidney transplant recipient successfully treated with tocilizumab and hydroxychloroquine. Am J Transplant. 2020;20(7):1902–6.
- Zhou D, Dai S-M, Tong Q. COVID-19: a recommendation to examine the effect of hydroxychloroquine in preventing infection and progression. J Antimicrob Chemother. 2020;75(7):1667–70.
- Fravel MA, Ernst M. Drug Interactions with Antihypertensives. Curr Hypertens Rep. 2021;23(3):1–8.
- Gautret P, Lagier J-C, Parola P, Meddeb L, Mailhe M, Doudier B, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. Int J Antimicrob Agents. 2020;56(1):105949.
AMU 2021. Volumen 3, Número 1
Fecha de envío: Fecha de aceptación: Fecha de publicación:
14/03/2021 04/04/2021 31/05/2021
Cita el artículo: Ramírez-García G, García-Molina P, Flor-Cremades M. C., Muñoz-Rojas B, Moleón-Moya J. Hidroxicloroquina y tocilizumab frente a COVID-19: un estudio observacional longitudinal. AMU. 2021; 3(1):24-39