Benites-Narziso, Gregorio¹; Redruello-Guerrero Pablo ² *; Pastor-Idoate, Salvador ¹⁻³
¹ Institute of Applied Ophthalmobiology (IOBA), University of Valladolid, 47011 Valladolid, Spain.
² Department of Ophthalmology, University Clinical Hospital of Valladolid, 47003, Valladolid, Spain.
³ Networks of Cooperative Research oriented to Health Results. RICORS- REI. National Institute of Health Carlos III, Madrid, Spain.
* Autor de correspondencia: benitesgregorio@gmail.com
Resumen
Introducción/Objetivos
El desprendimiento de retina es una emergencia medico-quirúrgica por su riesgo de pérdida visual, que necesita pronta intervención. El objetivo fue describir el perfil clínico de los pacientes con peores resultados visuales y evaluar el impacto del taponamiento con aceite de silicona.
Material y Métodos
Se realizo un estudio de cohortes retrospectivas analizándose las historias clínicas de pacientes que sufrieron un desprendimiento entre 2016 y 2019 en el Hospital Clínico Universitario de Valladolid. Se recogieron datos demográficos, presentacion en urgencias, parámetros quirúrgicos y agudeza visual al año. Se realizaron descripción de la muestra y un análisis bivariado según tipo de taponamiento.
Resultados
Se evaluaron 34 ojos, hubo distribución equitativa por género y mediana de edad de 55 años. La mediana de la mejor agudeza visual corregida preoperatoria fue de 0.7 logMAR (RIC: 0.4-2.0), con un 29.4% presentando un estado de mácula-ON y un 32.4% de pacientes pseudofaquicos. La mediana de agudeza visual postoperatoria mejor o a 0.2 logMAR (RIC: 0.1-0.5). Los agentes de taponamiento utilizados incluyeron C3F8 (55.9%), SF6 (17.6%) y aceite de silicona (26.5%). No se observaron diferencias significativas en la agudeza visual preoperatoria entre los grupos de taponamiento (p = 0.328). Se encontró una correlación negativa moderada entre la agudeza visual postoperatoria frente a la edad (r = -0.45, p = 0.007) y la agudeza visual preoperatoria (r = -0.48, p = 0.006).
Conclusiones
Los pacientes con peor AV preoperatoria mejoraron significativamente tras la cirug ́ıa. El aceite de silicona se
empleo con mayor frecuencia en pacientes mayores y no mostr ́ o diferencias significativas en el estado visual preoperatorio ni en el ́
resultado final frente a los taponamientos con gas. La recuperacion visual fue menor en pacientes de mayor edad. ́
Palabras clave: desprendimiento de retina, aceite de silicona, vitrectomía, agudeza visual.
Abstract
Introduction
Retinal detachment (RD) constitutes a medical-surgical emergency due to the potential visual impairment it may precipitate, which needs prompt intervention. The present study’s objective was to delineate the clinical profile of patients experiencing the most severe visual outcomes and assess the impact of silicone tamponade on the results obtained.
Materials and methods
A retrospective cohort study was conducted to analyze medical records of patients who experienced RD between 2016 and 2019 at the University Clinical Hospital of Valladolid. The variables collected encompassed demographic parameters, clinical presentations in the emergency department, surgical parameters, and visual outcomes at the one-year follow-up. The data analysis involved a comprehensive description of the sample and a bivariate analysis categorized by the type of tamponade utilized.
Results
A total of 34 eyes were evaluated, with equal distribution by gender and median age of 55 years. The median preoperative best corrected visual acuity (BCVA) was 0.7 logMAR (IQR: 0.4–2.0), with 29.4% presenting with macula-ON, 32.4% with pseudophakic status. Postoperative median BCVA improved to 0.2 logMAR (IQR: 0.1–0.5). Tamponade agents included C3F8 (55.9%), SF6 (17.6%), and silicone oil (26.5%). No significant differences were observed in preoperative VA across tamponade groups (p = 0.328). A moderate negative correlation was found between postoperative VA and age (r = –0.45, p = 0.007) and preoperative BCVA (r = –0.48, p = 0.006).
Conclusions
Patients with poorer preoperative visual acuity experienced significant postoperative improvement. Silicone oil was the preferred endo tamponade in older patients, showing no significant difference in preoperative visual status or final visual outcomes compared to gas tamponades. Older patients demonstrated less visual recovery, whereas those with worse initial visual acuity showed greater postoperative improvement.
Key words: retinal detachment, silicone oil, vitrectomy, visual acuity.
1. Introduction
Retinal detachment (RD), widely known as the separation of the neurosensory retina (NR) from the retinal pigmentary epithelium (RPE), represents a sight-threatening condition that can lead to permanent vision loss if not treated promptly (1). Its exact incidence and prevalence are currently difficult to know, despite the most common type (Rhegmatogenous RD or RRD) being estimated to occur in 1 in 10 000 patients (1). Primary rhegmatogenous RD requires urgent surgical intervention, and various techniques have been developed over the years. The selection of the most appropriate treatment remains a topic of considerable debate. The main surgical approaches include laser demarcation, pars plana vitrectomy (PPV), scleral buckling (SB), and pneumatic retinopexy (PR), each characterized by specific indications and limitations (1–4). PPV is often the default technique, particularly when no specific criteria favor other methods (1). While some expert guidelines suggest using it for elderly patients with multiple retinal tears (4).
Gas is the most commonly used tamponade agent due to its high surface tension and gradual resorption. However, air travel and high-altitude changes are contraindications to its use (1). Silicone oil (SO) is often reserved for patients who cannot maintain prone positioning or require air travel and for cases with inferior retinal breaks (4). While SO provides a shorter visual recovery time and does not dissolve, its removal can be challenging, and unexplained vision loss postoperatively has been reported (1).
The most appropriate surgical technique selection depends on several factors, including patient-specific characteristics (age, myopia status, history of prior ocular surgery or trauma, and family history) and RD-specific features (location, number of breaks, and extent of detachment) (1,5). Multiple studies have been conducted to compare the outcomes and efficacy of the various approaches available (6–8). However, there are no universally accepted guidelines or consensus-based protocols for determining the best approach, leaving the decision mainly to the surgeon’s clinical judgment, which ultimately accentuates the heterogeneity of the protocols in different medical settings (1,5). Given the ongoing debate regarding the optimal surgical strategy and choice of tamponade, this study aimed to contribute to the knowledge gap by analyzing the clinical profile of patients with RD who have poorer visual outcomes and evaluating the impact of silicone oil tamponade on postoperative results in a retrospective cohort from our institution.
2. Materials and methods
A retrospective cohort study analyzed the medical records of patients who suffered from RD between 2016 and 2019 at the Hospital Clínico Universitario de Valladolid Medical Center, following them for one year after diagnosis. The variables collected included demographic parameters (such as age, and sex), clinical presentation in the emergency department (affected eye, visual acuity (VA) at presentation, whether the macula was affected, whether the patient had pathological myopia, whether the patient was phakic, whether the patient had vitreoretinal proliferation, days since the onset of symptoms and days until surgery), surgical parameters (such as the number of retinal tears identified in the operating room, the number of laser impacts that occurred, the type of tamponade used, whether scleral buckle was used, whether phacoemulsification was performed during surgery and whether retinectomy was performed) and functional outcomes (VA, whether there was a re-RD, whether cataracts developed and whether they were operated on if necessary) at one year of follow-up. VA was converted to a logarithmic scale and reported as the logarithm of the minimum angle of resolution (logMAR).
Data analysis included a description of the sample. The cohort exposed to treatment with silicone oil tamponade was compared with the cohort that had gas tamponade. A bivariate analysis based on the endotamponade used was performed. In addition, correlation analyses were performed between the difference in VA before and after the intervention and the days until surgery. Finally, a Pearson correlation was performed to analyze the relationship between different variables.
The center’s Research Ethics Committee approved the performance of this study.
3. Results
The number of eyes that underwent DR and were collected was 34. Descriptive data of the sample are presented in Table 1. An equal distribution by gender (50% male and 50% female) and a median age of 55 years (IQR: 52-67) was observed. Ocular involvement was slightly more frequent in the right eye (52.9%). Preoperative visual status showed a median VA of 0.7 logMAR (IQR: 0.4-2.0), with macular-ON status in 29.4% of cases. The median time to surgery was 6 days (IQR: 4-8), while symptoms were present for a median of 2 days (IQR: 0-5) before surgical management. Pseudophakia (32.4%) and pathological myopia (35.3%) stood out as relevant comorbidities, while the median number of retinal breaks was 2 (IQR: 1-4). Surgical strategies included median laser impacts of 709 (IQR: 410-1414), scleral buckling in 29.4% of cases, and various endotamponades (perfluoropropane (C3F8) in 55.9%, sulfur hexafluoride (SF6) in 17.6%, and silicone in 26.5%). Postoperative visual outcomes revealed an improvement in median VA to 0.2 logMAR (IQR: 0.1-0.5), with a VA difference of -0.1 logMAR (IQR: -0.4-0.2), indicating a significant clinical benefit in most cases. Complications included proliferative vitreoretinopathy (PVR) recurrence (14.7%) and the presence of cataracts (8.8%).
Table 1. Collected sample description.
| Variables | Count |
| Sex | |
| Male | 17 (50%) |
| Female | 17 (50%) |
| Age (median (IQR)) | 55 (52-67) |
| Eye | |
| OD | 18 (52.9%) |
| OS | 16 (47.1%) |
| VA pre in logMAR (median (IQR)) | 0.7 (0.4-2) |
| Macula ON | 10 (29.4%) |
| Fóvea ON | 13 (38.2%) |
| Days until surgery (median (IQR)) | 6 (4-8) |
| Pseudophakic | 11 (32.4%) |
| Days of sice onset symptoms (median (IQR)) | 2 (0.0-5) |
| Pre-PVR | 2 (5.9%) |
| Phathologic myopia | 12 (35.3%) |
| Nº breaks (median (IQR)) | 2 (1-4) |
| Laser impacts (median (IQR)) | 709 (410-1,414) |
| Scleral Buckle | 10 (29.4%) |
| Type of Endotamponator | |
| C3F8 | 19 (55.9%) |
| SF6 | 6 (17.6%) |
| Silicone | 9 (26.5%) |
| Associated Phaco | 17 (50%) |
| Retinectomy | 4 (11.8%) |
| VA post logMAR (median (IQR)) | 0.2 (0.1-0.5) |
| VA differences logMAR (median (IQR)) | -0.1 (-0.4-0.2) |
| VRP-recidive | 5 (14.7%) |
| Presence of cataract | 3 (8.8%) |
| Phacoemulsification Post | 1 (2.9%) |
| Presence of PVR | 1 (2.9%) |
| Total | 34 (100%) |
IQR: interquartile range, OD: Oculus dexter, OS: Oculus sinister, PVR: proliferative vitreoretinopathy, C3F8: perfluoropropane, SF6: sulfur hexafluoride, VA: visual acuity, logMAR: Logarithm of the Minimum Angle of Resolution.
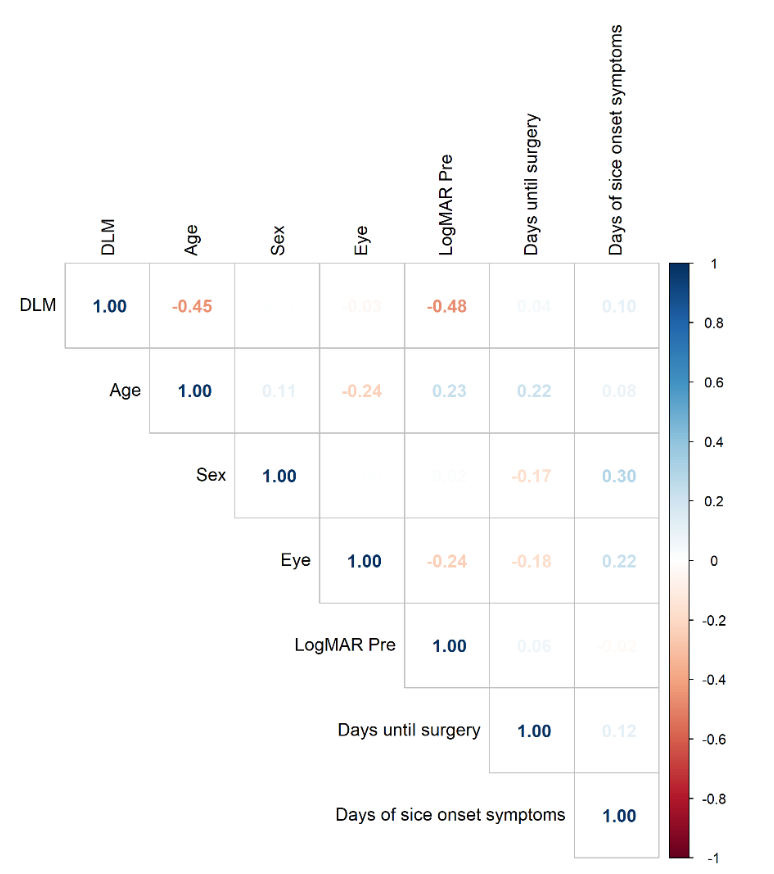
Bivariate analysis (Table 2) of the different endotamponades showed statistically significant age differences (p = 0.029) and the presence of PVR (p = 0.018). Patients treated with silicone were significantly older (median: 70 years (IQR: 57-73)) compared with those in C3F8 (54 years (IQR: 49.5-55.5)) and SF6 (63 years (IQR: 54.5-70.0)). Although no significant differences were found in preoperative VA (p = 0.328), patients treated with SF6 showed worse initial VA (median: 2.7 logMAR (IQR: 1.8-3.0)) compared with C3F8 (0.7 logMAR (IQR: 0.3-1.5)) and silicone (0.5 logMAR (IQR: 0.4-1.3)). Despite these initial differences, postoperative VA did not vary significantly between groups (p = 0.515). The incidence of preoperative PVR was low overall but more prevalent in patients treated with SF6 (33.3%), and residual PVR was significantly higher in the silicone group (12.5%, p = 0.018). The Pearson correlation analysis between the difference in VA measured in logMAR can be seen in Figure 1. A moderately negative correlation with age is shown (r = -0.45, p = 0.007). Likewise, a moderately negative correlation is presented with the previous value of VA (r = -0.48, p = 0.006).
Table 2. Bivariate analysis comparing the different endotamponades used in surgery. * Statistically significant test. $ median (IQR).
| Variables | C3F8 | SF6 | Silicone | p-value |
| Sex | 0.225 | |||
| Male | 7 (36.8%) | 4 (66.7%) | 6 (66.7%) | |
| Female | ||||
| Age $ | 54 (49.5-55.5) | 63(54.5-70) | 70 (57-73) | 0.029* |
| Eye | 0.126 | |||
| OD | 13 (68.4%) | 2 (33.3%) | 3 (33.3%) | |
| OS | 6 (31.6%) | 4 (66.7%) | 6 (66.7%) | |
| VA pre $ | 0.7 (0.3-1.5) | 2.7 (1.8-3) | 0.5 (0.4-1.3) | 0.328 |
| Macula ON | 7 (36.8%) | 2 (33.3%) | 1 (12.5%) | 0.447 |
| Fóvea ON | 10 (76.9%) | 2 (50%) | 1 (12.5%) | 0.282 |
| Days until surgery $ | 6 (3.5-8) | 5.5 (5-10.5) | 6 (6-8) | 0.909 |
| Pseudophakic | 5 (26.3%) | 2 (33.3%) | 4 (44.4%) | 0.631 |
| Days since onset of symptoms $ | 2 (0-5) | 3.5 (0.8-1) | 1 (0.3-1.8) | 0.478 |
| Pre-PVR | 0 (0%) | 1 (33.3%) | 1 (12.5%) | 0.258 |
| Phathologic myopia | 7 (58.3%) | 3 (100%) | 2 (66.7%) | 0.392 |
| Nº breaks $ | 2 (1-4.5) | 3 (1.5-3) | 2 (1-2.5) | 0.885 |
| Laser impacts $ | 816 (374.8-1 538) | 1,062 (779-1 562.5) | 522 (428-613.3) | 0.231 |
| Scleral Buckle | 6 (40%) | 1 (16.7%) | 3 (33.3%) | 0.592 |
| Associated Phaco | 8 (42.1%) | 4 (66.7%) | 5 (55.6%) | 0.535 |
| Retinectomy | 4 (33.3%) | 0 (0%) | 0 (0%) | 0.076 |
| VA post $ | 0.2 (0.1-0.4) | 0.2 (0-0.6) | 0.4 (0.1-1.3) | 0.515 |
| VA difference $ | -0.1 (-0.2-0.4) | -0.2 (-0.6- -0.1) | -0.1 (-0.9-0.2) | 0.636 |
| PVR-recidive | 3 (27.3%) | 1 (16.7%) | 1 (12.5%) | 0.827 |
| Presence of cataract | 3 (15.8%) | 0 (0%) | 0 (0%) | 0.273 |
| Phacoemulsification Post | 1 (5.3%) | 0 (0%) | 0 (0%) | 0.666 |
| Presence of PVR | 0 (0%) | 0 (0%) | 1 (12.5%) | 0.018* |
| Total | 19 (100%) | 6 (100%) | 9 (100%) |
C3F8: perfluoropropane, SF6: sulfur hexafluoride, OD: Oculus dexter, OS: Oculus sinister, VA: visual acuity, PVR: proliferative vitreoretinopathy.
$: surgery.
Figure 1. Pearson correlation analysis between the difference in VA (DLM) and different clinical variables.
4. Discusion
The controversy surrounding RD management extends beyond the chosen surgical technique to the agents and variants performed (9,10). Our study found that patients’ profiles were similar in gender distribution, predominantly late-middle-aged, with a slightly higher frequency of right-sided affection and fewer retinal breaks. Other studies (7,8,11–13) have reported variable results, and some align with ours.
Preoperatively, our cohort exhibited moderate visual impairment (0.7 logMAR) in our series, and the majority had macular involvement. Ultimately, our postoperative visual outcomes were satisfactory (0.2 logMAR) and significant. Sakamoto et al., in a large cohort, showed a considerably better preoperative VA than ours (mean best corrected visual acuity (BCVA) of -0.26 ± 0.91 logMAR), and just 48% had macula OFF status (12). Their final report, ruled by Baba et al., showed an overall BCVA of 0.10 ± 0.32 logMAR (14). Their surgery was performed 2 days longer than ours (12). Although this waiting time may be a concerning fact, it is still not clear that a shorter waiting time for surgery, regardless of the macula status, is related to better visual outcomes in the long term; however, it is suggested (15). A similar big report by Ryan et al., and Joseph et al., showed preoperative BCVA values estimated from 0.0 to 2.0 logMAR for phakic and approximately 1.03 (0.18 to ~2.0) logMAR for pseudophakic patients, with consequent estimated postoperative results of 0.0 to 1.0 logMAR and 0.34 (0.15 to ~1.4) logMAR, respectively (16,17). Gonzalez-Lopez et al., who worked with an older patient cohort undergoing PPV, reported an approximate preoperative BCVA of 1.3–1.4 logMAR, worse than ours, with a postoperative success of approximately 1.0 logMAR (13). Echegaray et al., compared PPV alone or in combination with SB and reported significant macular impairment (74%), preoperative BCVA of 1.057 logMAR, and a postoperative BCVA of 0.52 logMAR in the long term (18). These findings illustrate the variability among studies, as authors select different variables and associations, complicating the establishment of standardized management protocols.
Approximately one-third of our patients underwent SB, and no statistical difference was found when analyzing different endo tamponade agents in those cases. Lena et al., in a recent systematic review, compared the outcomes between using PPV alone and combined with SB, reporting similar baseline and postoperative BCVA without a statistically significant difference between the two groups (p = 0.310) (7).
The fact that pseudophakia and pathological myopia represent important conditions in our study drives our attention. These conditions present variably compared with other authors’ findings, like Sakamoto et al. (81.8% phakic) (12), Gonzalez-Lopez et al. (53,8% pseudophakic) (13), Heydinger et al. (60.9% myopic, 63.1% phakic) (9), and Echegaray et al. (59% pseudophakic) (18). This represents the variability of the different populations and the need for a clearer and broader analysis of all these factors and their association with the outcomes, as the phakic condition is considered highly relevant in management. Gibelalde et al. reported that pseudophakic patients present with multiple and inferior detachments, more retinal tears, and a tendency to present with macular involvement (11).
Regarding comparing endotamponade strategies, C3F8 was the most used (55.9%), and statistically significant features were associated with it. The more aged (p = 0.029) the patient, the more they tended to undergo C3F8, SF6, and silicone tamponade, respectively, with the latter being associated with the presence of PVR (p = 0.018) despite being presented with low overall incidence and higher in patients treated with SF6 (33.3%). Despite differences in BCVA between these groups, the association wasn’t statistically significant either pre- or postoperatively. These findings align with those of Tanriverdi et al. (p = 0.080), who compared C3F8 versus SO (19), as well as with Heydinger et al. (9), who analyzed the same tamponade agents we used. In contrast, Huang et al. reported significantly better postoperative visual acuity with gas tamponade than with silicone oil (0.53 ± 0.55 logMAR vs. 0.70 ± 0.69 logMAR, p = 0.002). However, both agents had similar overall visual recovery rates (6). Additionally, Tzoumas et al., in a large multicenter cohort, found that denser silicone oil achieved better anatomical and visual success than lighter silicone oil in eyes with inferior retinal breaks and PVR-C (8).
Our study also found that older patients experienced less visual recovery after surgery. Conversely, patients with poorer initial vision (higher logMAR values) exhibited greater postoperative improvement, contrasting with findings by Gonzalez-Lopez et al. (13), who reported the opposite trend. Lena et al. (7), identified macula-off status, pre-existing PVR, and detachment extent as factors associated with worse outcomes, though they concurred with our findings regarding the effect of age. Similarly, Treder et al. (20), reported that BCVA \textgreater{}0.3 logMAR, female gender, and silicone oil tamponade were linked to poor visual outcomes.
Our study offers a new perspective, focusing on the group of patients with the poorest outcomes. Additionally, makes a comparison of patients based on the treatment received. One of our primary limitations was the lack of long-term postoperative follow-up. Additionally, we did not stratify patients by the etiology of their RD, which could have helped establish stronger associations between variables and refine patient management strategies. Finally, we did not include anatomical success rates, which would provide a more comprehensive assessment of surgical efficacy. These considerations should be duly acknowledged in future research endeavors. It is recommended that larger studies encompassing a more diverse spectrum of patient groups be conducted to enhance the development of subsequent guidelines on the subject.
5. Conclusions
Patients with poorer preoperative visual acuity experienced significant postoperative improvement, often presenting with moderate visual impairment and substantial macular involvement before surgery. Silicone oil was the preferred endotamponade in older patients, showing no significant difference in preoperative visual status or final visual outcomes compared to gas tamponades. However, its use was associated with a higher incidence of postoperative proliferative vitreoretinopathy. Older patients demonstrated less visual recovery, whereas those with worse initial visual acuity (higher logMAR values) showed greater postoperative improvement.
Declarationes
Acknowledgements
We thank the patients and the institutions involved, the Hospital Clínico Universitario de Valladolid (HCUV) and the Instituto de Oftalmobiología Aplicada (IOBA), for their collaboration and support in the development of this work.
Conflicts of interest
The authors declare no conflict of interest.
Funding
The authors declare that no funding was received for the conduct of this study.
Referencias
1. Lin JB, Narayanan R, Philippakis E, Yonekawa Y, Apte RS. Retinal detachment. Nat Rev Dis Primers 2024;10:1–13.
2. Warren A, Wang DW, Lim JI. Rhegmatogenous retinal detachment surgery: A review. Clin Exp Ophthalmol 2023;51:271–9.
3. Feltgen N, Callizo J, Hattenbach LO, Hoerauf H. The urgency of surgical treatment for rhegmatogenous retinal detachment. Ophthalmologe 2021;118:160–5.
4. Huang Y Te, Yang CH, Chen SJ, Cheng CK, Ho TC, Wu TT, et al. Guidelines and treatment patterns for primary rhegmatogenous retinal detachments: Expert consensus and survey in Taiwan Retina Society. J Chin Med Assoc 2024;87:25–32.
5. Quiroz-Reyes MA, Babar ZUD, Hussain R, Loh ZC, Quiroz-Gonzalez EA, Quiroz-Gonzalez MA, et al. Management, risk factors and treatment outcomes of rhegmatogenous retinal detachment associated with giant retinal tears: scoping review. Int J Retina Vitreous 2024;10.
6. Huang RS, Mihalache A, Lau THA, Popovic MM, Kertes PJ, Muni RH. Pars Plana Vitrectomy With Silicone Oil or Gas Tamponade for Uncomplicated Retinal Detachment: A Systematic Review and Meta-Analysis. Am J Ophthalmol 2024;266:144–55.
7. Lena ER, Patil NS, Popovic MM, Eshtiaghi A, Dhoot AS, Muni RH, et al. Evaluation of Pars Plana Vitrectomy With and Without Supplemental Scleral Buckle for the Repair of Rhegmatogenous Detachment Due to Inferior Retinal Breaks: A Systematic Review. Ophthalmic Surg Lasers Imaging Retina 2025;56:37–45.
8. Tzoumas N, Yorston D, Laidlaw DAH, Williamson TH, Steel DH, Ellabban AA, et al. Improved Outcomes with Heavy Silicone Oil in Complex Primary Retinal Detachment: A Large Multicenter Matched Cohort Study. Ophthalmology 2024;131:731–40.
9. Heydinger S, Wang AL, Ufret-Vincenty R, Robertson ZM, He YG. Comparison of Surgical Outcomes for Uncomplicated Primary Retinal Detachment Repair. Clin Ophthalmol 2023;17:907–15.
10. Popovic MM, Muni RH, Nichani P, Kertes PJ. Pars plana vitrectomy, scleral buckle, and pneumatic retinopexy for the management of rhegmatogenous retinal detachment: a meta-analysis. Surv Ophthalmol 2022;67:184–96.
11. Gibelalde A, Pinar-Sueiro S, Ibarrondo O, Martínez-Soroa I, Mendicute J, Ruiz Miguel M. Are all primary retinal detachments the same? Anatomic and functional differences between phakic and pseudophakic patients. Int J Retina Vitreous 2023;9:17.
12. Sakamoto T, Kawano S, Kawasaki R, Hirakata A, Yamashita H, Yamamoto S, et al. Japan-Retinal Detachment Registry Report I: preoperative findings in eyes with primary retinal detachment. Jpn J Ophthalmol 2020;64:1–12.
13. Gonzalez-Lopez JJ, Arruza Santos ME, Leon Garcia J. Pars plana vitrectomy in patients aged 85 years and older: a single-centre, retrospective cohort study. Int Ophthalmol 2023;43:4887–96.
14. Baba T, Kawasaki R, Yamakiri K, Koto T, Nishitsuka K, Yamamoto S, et al. Visual outcomes after surgery for primary rhegmatogenous retinal detachment in era of microincision vitrectomy: Japan-Retinal Detachment Registry Report IV. Br J Ophthalmol 2021;105:227–32.
15. Sothivannan A, Eshtiaghi A, Dhoot AS, Popovic MM, Garg SJ, Kertes PJ, et al. Impact of the Time to Surgery on Visual Outcomes for Rhegmatogenous Retinal Detachment Repair: A Meta-Analysis. Am J Ophthalmol 2022;244:19–29.
16. Ryan EH, Ryan CM, Forbes NJ, Yonekawa Y, Wagley S, Mittra RA, et al. Primary Retinal Detachment Outcomes Study Report Number 2: Phakic Retinal Detachment Outcomes. Ophthalmology 2020;127:1077–85.
17. Joseph DP, Ryan EH, Ryan CM, Forbes NJK, Wagley S, Yonekawa Y, et al. Primary Retinal Detachment Outcomes Study: Pseudophakic Retinal Detachment Outcomes: Primary Retinal Detachment Outcomes Study Report Number 3. Ophthalmology 2020;127:1507–14.
18. Echegaray JJ, Vanner EA, Zhang L, Fortun JA, Albini TA, Berrocal AM, et al. Outcomes of Pars Plana Vitrectomy Alone versus Combined Scleral Buckling plus Pars Plana Vitrectomy for Primary Retinal Detachment. Ophthalmol Retina 2021;5:169–75.
19. Tanriverdi A, Ozer O, Eroz P, Dinc E, Dursun O, Adiguzel U. Comparison of anatomical and functional outcomes of pars plana vitrectomy for rhegmatogenous retinal detachment with phaco-vitrectomy. Ret-Vit 2024;33:112–6.
20. Poulsen CD, Green A, Grauslund J, Peto T. Long-Term Outcome of Patients Operated with Pars Plana Vitrectomy for Primary Rhegmatogenous Retinal Detachment. Ophthalmic Res 2020;63:25–33.
AMU 2026. Volumen 8, Número 1
Fecha de envío: 18/02/2025
Fecha de aceptación: 05/03/2025
Fecha de publicación: 18/04/2025
Cita el artículo: Benites-Narcizo G, Redruello-Guerrero P, Pastor-Idoate S. CEvaluation of visual outcomes in patients with retinal
detachment: a retrospective cohort study. AMU. 2026; 8(1):56-61